Return to Diagnostic Studies
Page
Return to
Chelation Therapy Page
Challenge
Results
In interpreting the challenge results, please understand that the findings,
the "spills:, reflect not just your body burden of a given metal, but which
chelating agent we used, and at what strength it was administered (discussed
elsewhere on this site). The "within reference range", elevated", and
"very elevated" ranges refer to non-provoked urine metal levels. The
challenge results depict provoked levels, so don't become overly alarmed when
your results are in the "elevated range". We use the non-provoked
parameters because there are no standardized "normal" or "abnormal" ranges for
provoked specimens. We need to remember that a truly normal level for a
toxic metal would have to be zero, non-detectable.
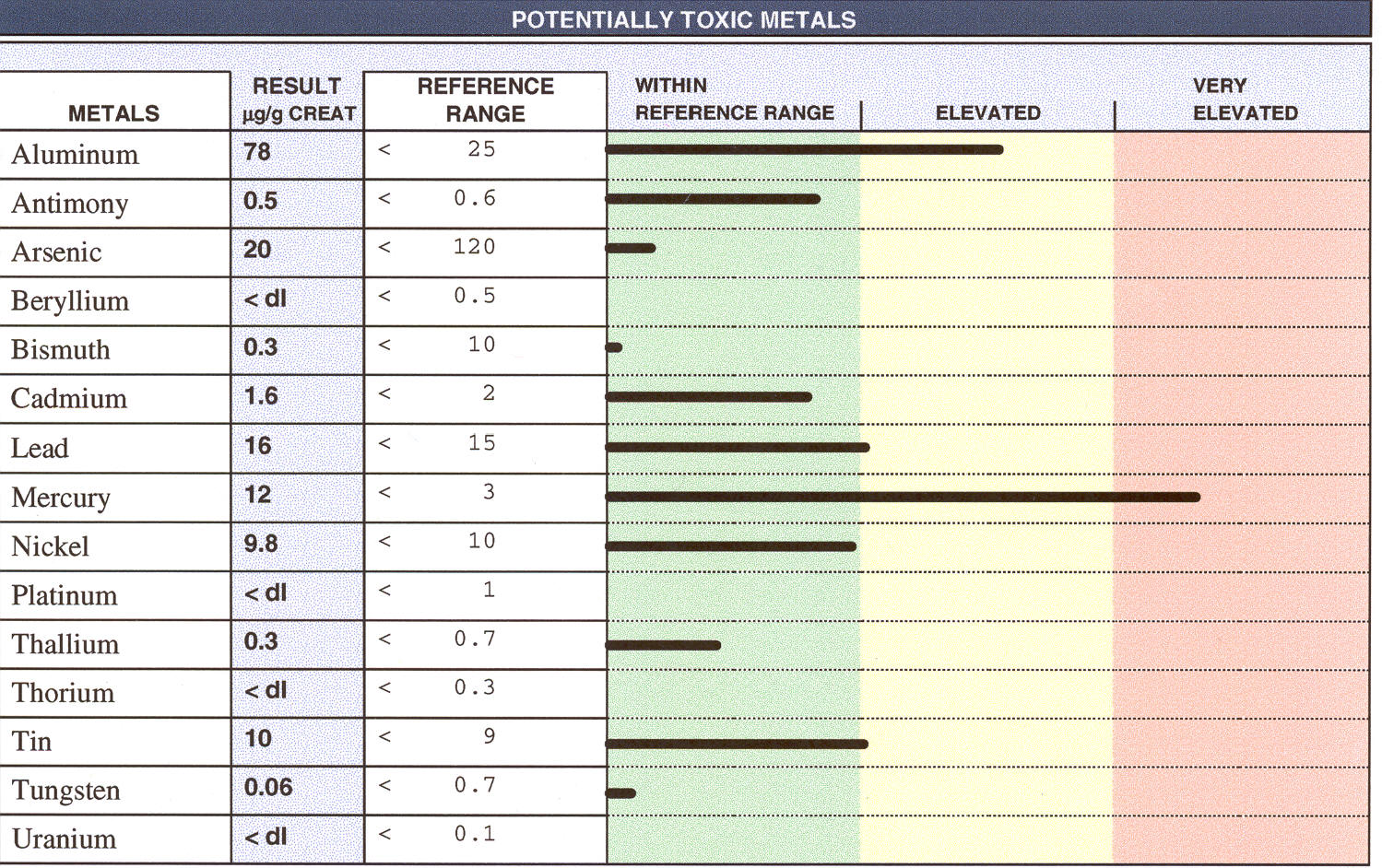 This
triple challenge demonstrates predominant spills of Aluminum and Mercury.
Aluminum can be chelated out with Desferoxamine and EDTA (with glycine loading),
but is not removed with di-thiol agents, such as DMPS and DMSA. Mercury,
on the other hand, is not removed with EDTA, but can be chelated out with DMSA
and DMPS. This patient would need a two pronged, or staged approach to
achieve complete toxic metal detoxification.
This
triple challenge demonstrates predominant spills of Aluminum and Mercury.
Aluminum can be chelated out with Desferoxamine and EDTA (with glycine loading),
but is not removed with di-thiol agents, such as DMPS and DMSA. Mercury,
on the other hand, is not removed with EDTA, but can be chelated out with DMSA
and DMPS. This patient would need a two pronged, or staged approach to
achieve complete toxic metal detoxification.
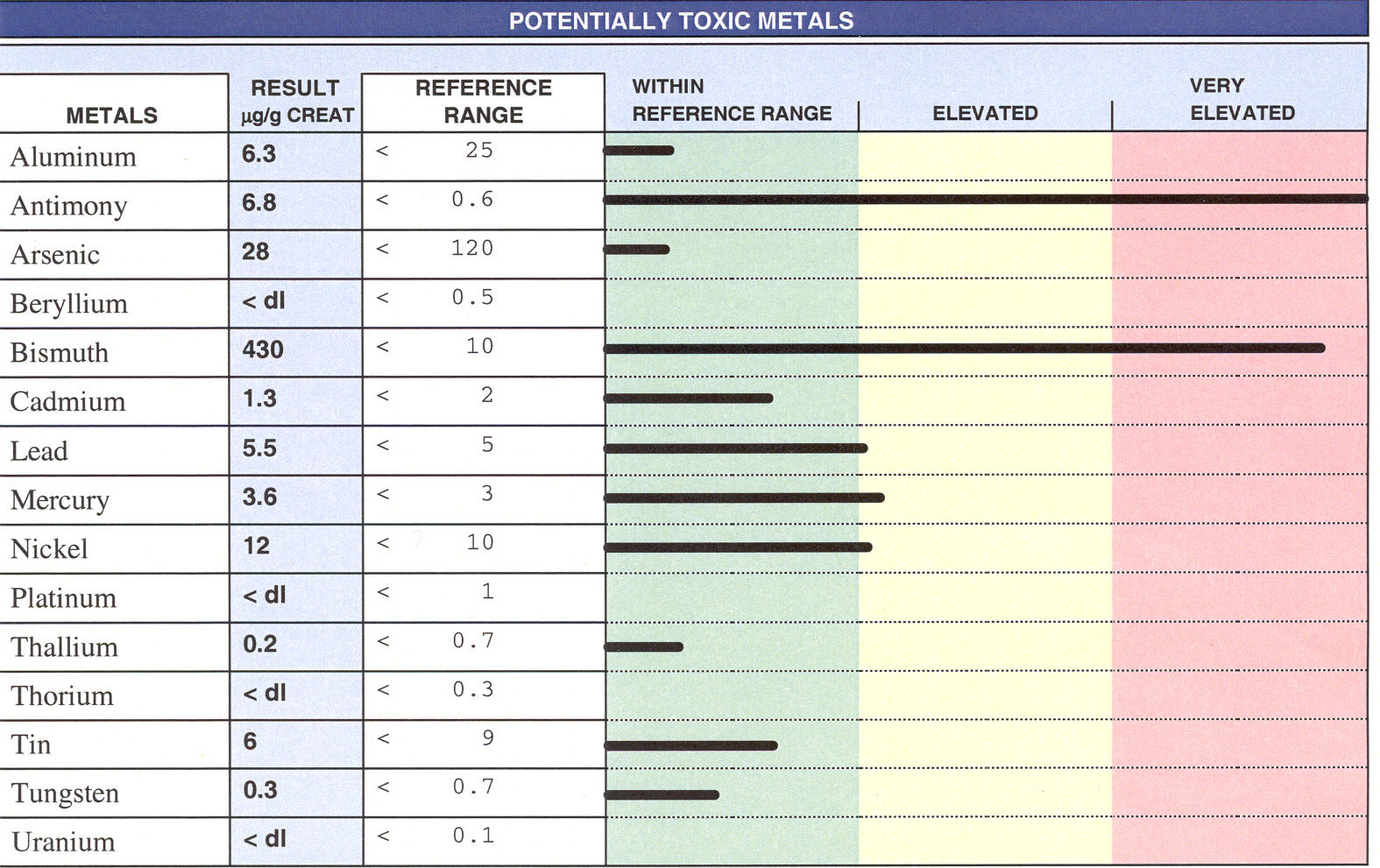 This
rather unusual challenge result demonstrates spills of Antimony and Bismuth.
Bismuth is felt to be relatively innocuous, while Antimony has been implicated
in a number of disease states, including crib death and cardiomyopathy.
This
rather unusual challenge result demonstrates spills of Antimony and Bismuth.
Bismuth is felt to be relatively innocuous, while Antimony has been implicated
in a number of disease states, including crib death and cardiomyopathy.
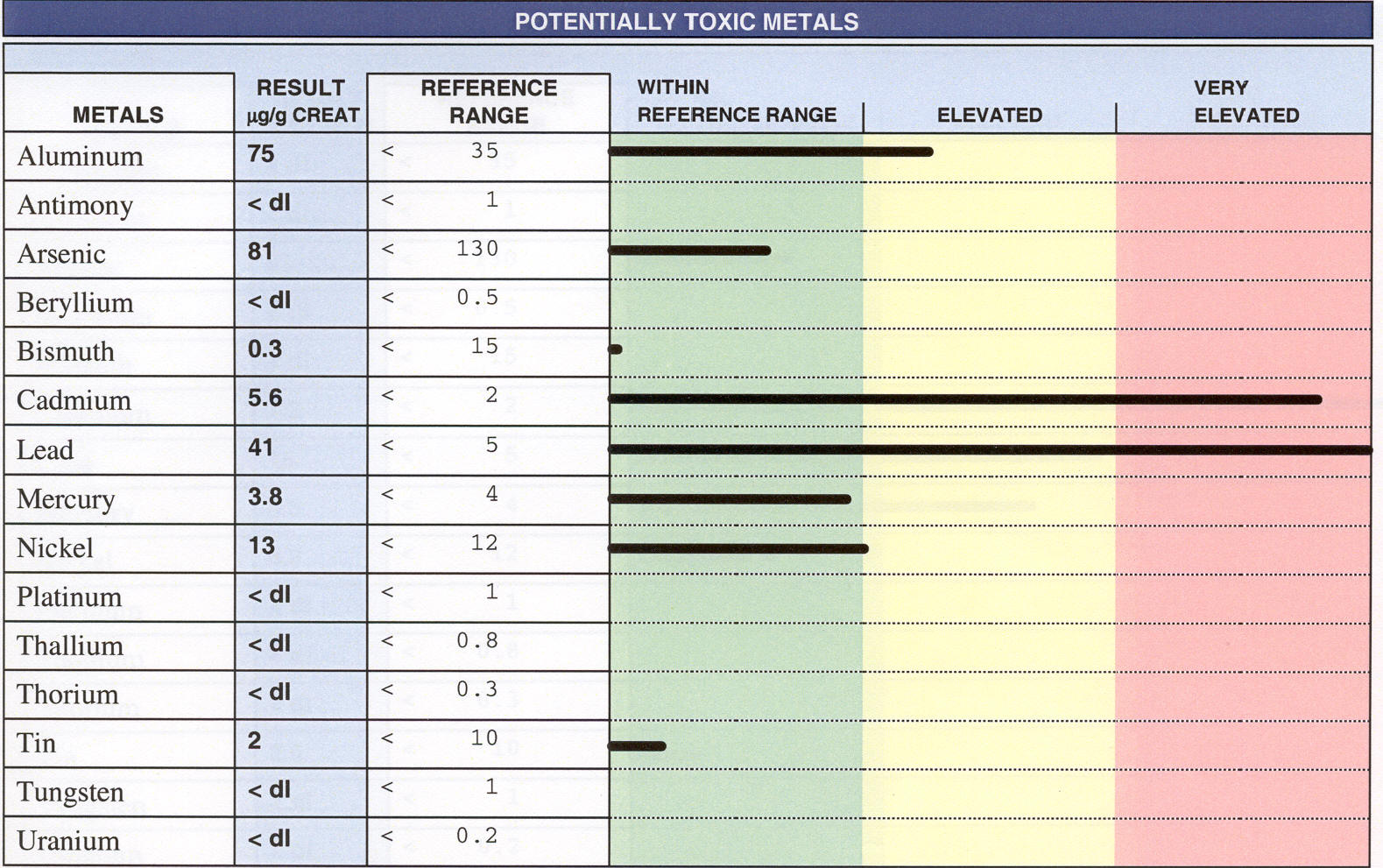 This
challenge brought out heavy spills of Lead and Cadmium, with detectible but less
impressive spills of Aluminum, Mercury, and Nickel. EDTA and DMSA would be
the chelators of choice for this patient.
This
challenge brought out heavy spills of Lead and Cadmium, with detectible but less
impressive spills of Aluminum, Mercury, and Nickel. EDTA and DMSA would be
the chelators of choice for this patient.
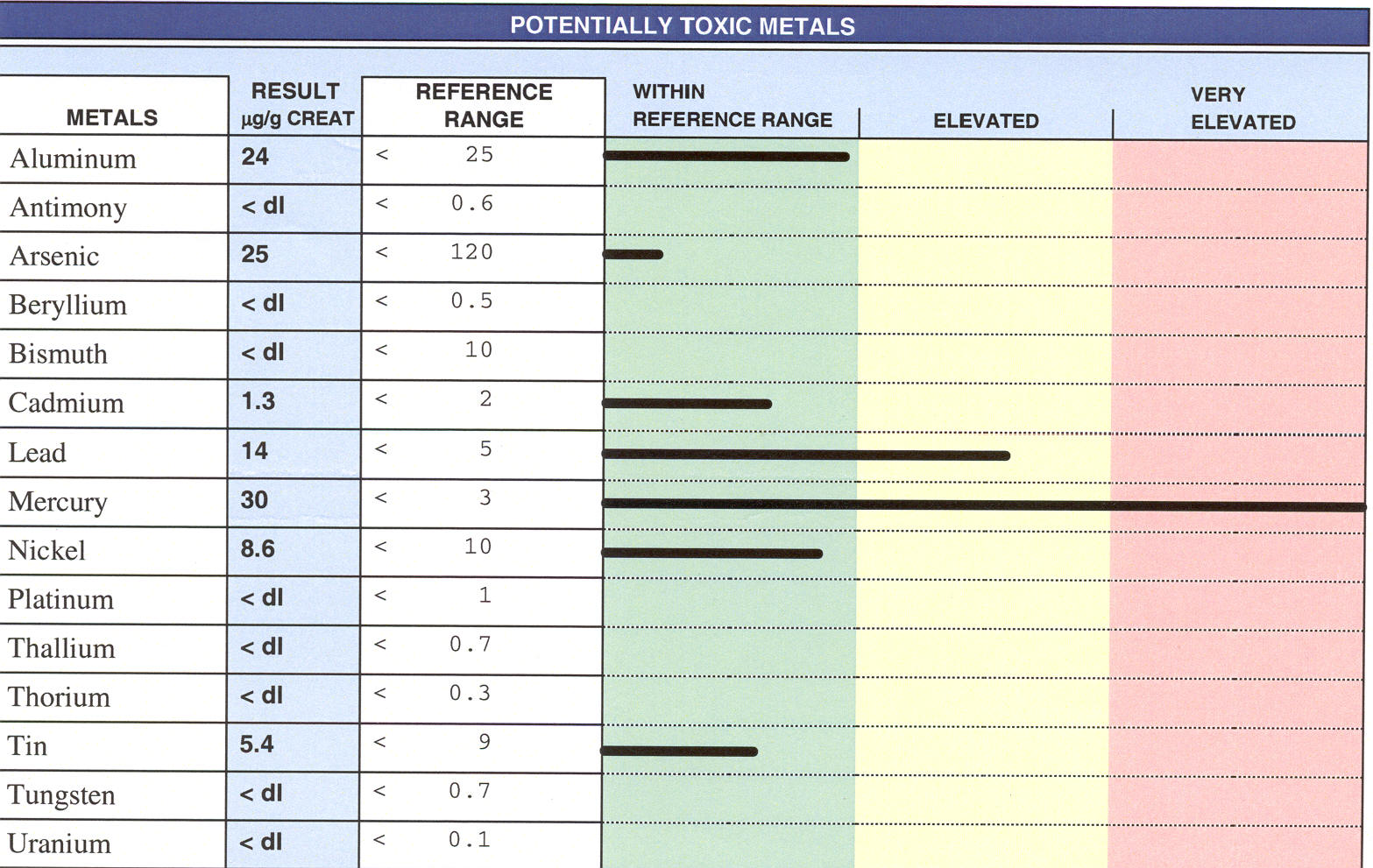
A
predominant Mercury spill is seen, with lesser amounts of Lead and Aluminum.
DMPS is our most effective Mercury chelator and will also bind Lead. DMSA
would be the second choice, but it is quantitatively less effective than is
DMPS. EDTA monotherapy would be inappropriate as EDTA is not an effective
Mercury chelator.
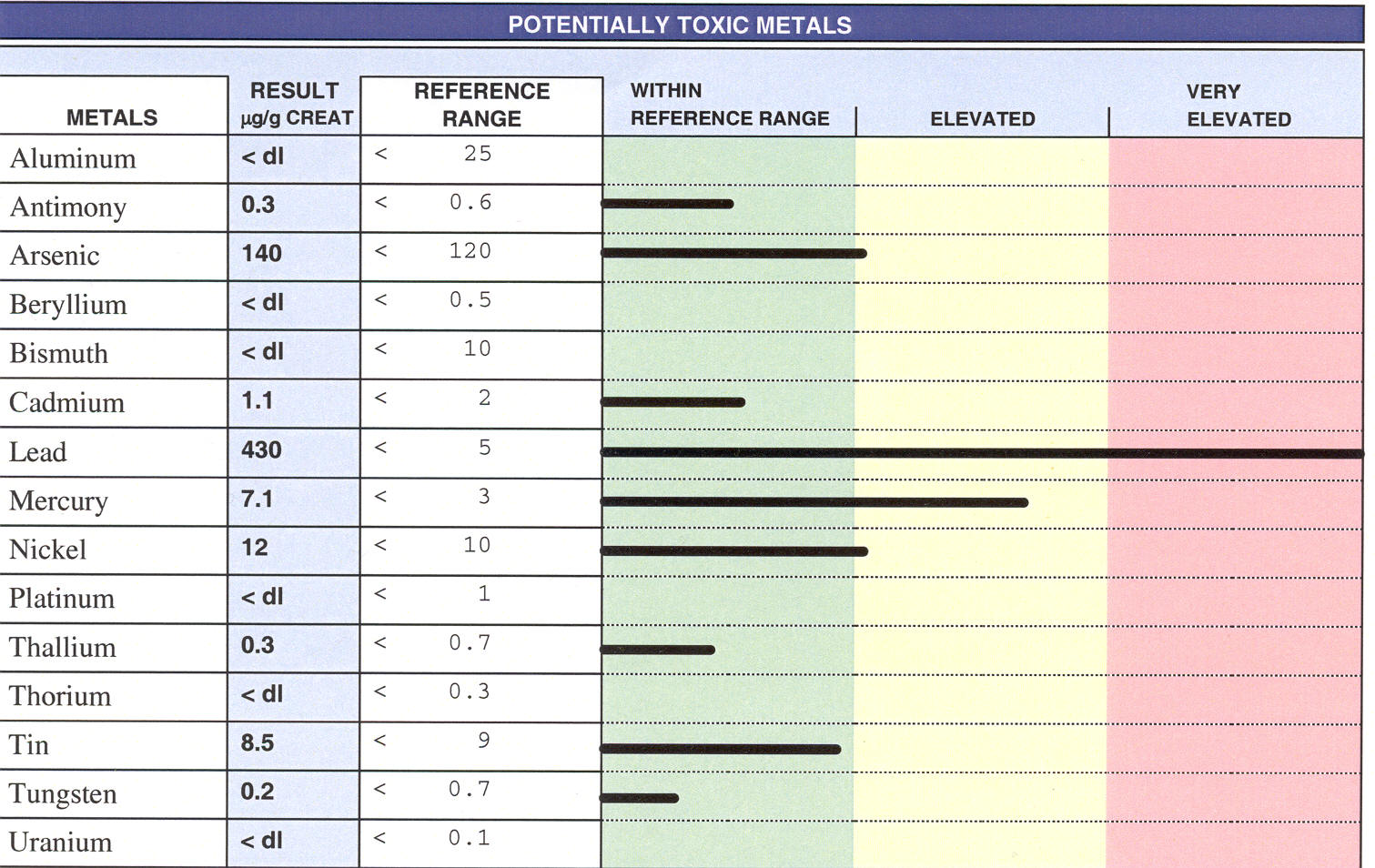
This is the greatest Lead spill that I have seen following a triple
challenge. IV EDTA, either Calcium or Magnesium EDTA makes sense here,
combined with oral EDTA and Zeolite. LED for Lead (new to me as of late '06) may
also be applied once I gain competence in this technology)
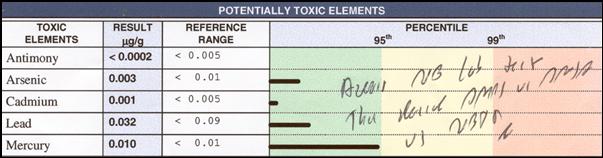 Blood levels of a given metal do not correlate well with tissue levels, with
your body burden of that metal. Red cells survive in the circulation for
90 days. Red cell metal analysis gives us a fairly good indicator of your
nutritional mineral status, and reflects "what has been floating around" over
the past three months. However, as a measure of toxic metal body burden,
the red cell analysis
Blood levels of a given metal do not correlate well with tissue levels, with
your body burden of that metal. Red cells survive in the circulation for
90 days. Red cell metal analysis gives us a fairly good indicator of your
nutritional mineral status, and reflects "what has been floating around" over
the past three months. However, as a measure of toxic metal body burden,
the red cell analysis 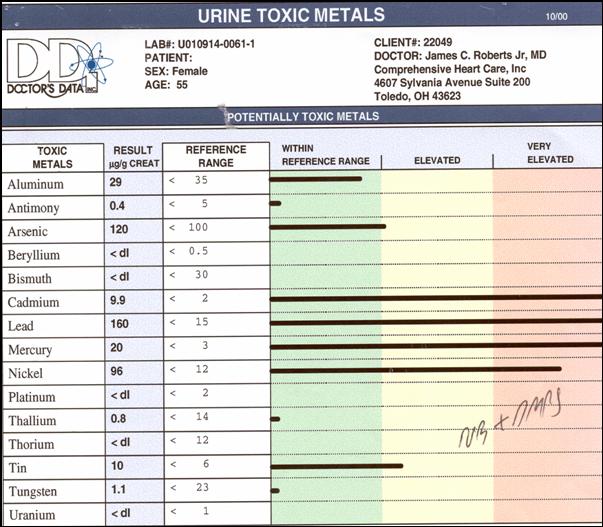 is
limited. The red cell study at your left suggests an isolated problem with
Mercury.
is
limited. The red cell study at your left suggests an isolated problem with
Mercury.
However, a double challenge (IV DMPS and rectal EDTA) carried out on
the same patient demonstrated huge spills of Lead and Cadmium, along with the
Mercury picked up on the red cell study. This is why we rely on challenge
study results in decision making.