
Return to CHC Home Page
Return to Diagnostic Studies
Estrogen Metabolism
within the framework of
Bioidentical Ovarian Hormone Replacement Therapy (HRT)
Optimal health requires a sustained and balanced interaction between peptide (thyroid, pancreatic, and neural) and steroid (gonadal, adrenal, and neural) hormones. Advancing age, nutritional imbalance, chronic stress, and the effects of commonly prescribed medications lead to imbalances and deficiencies, conditions that we can address with orthomolecular* bioidentical HRT. For optimal results, it is important that clinicians and patients understand hormonal physiology, its normal balancing mechanisms, and the clinical trials of HRT efficacy and safety.
Why should we replace ovarian hormones (or androgens in men)? The answer: to
make you feel better, live better, and live longer. While it might sound trite,
we really are as young as our hormones. Conversely, as we lose hormonal
support, health decline begins. As ovarian hormone levels decreases, we see
(and you experience):
A. An increase in LDL and Lp(a) cholesterol, along with an increase in clot
promoting factors such as fibrinogen, PAI-1, and Factor VII. CV risk increases
such that by age 65 a woman's risk rises to that of an age-matched man.
B. Accelerated bone demineralization, coupled with decreased Vitamin D activation
and calcium absorption, increasing risk of osteoporotic fracture.
C. Hot flashes, mood swings, insomnia, weight gain, fluid retention, and reduced
libido.
While you may seek HRT to deal with these quality of life effects (and why not – life is to be enjoyed, not suffered), our interest is in attenuating the negative health effects associated with hormonal insufficiency. To accomplish this, and with maximal safety, you need to be acquainted with hormonal physiology (and your physicians must understand this science in detail).
The ovaries (and adrenal glands, via aromatization of testosterone) release three estrogen species, along with progesterone, into the blood stream. These fat soluble (and water insoluble) molecules cannot dissolve in blood; instead they attach to a transport protein (SHBG, sex hormone binding globulin) allowing them to circulate to peripheral cells. Upon contact with a cell capable of responding to hormonal stimulation, the estrogen molecule is released by SHBG, and is then translocated across the cell membrane and into the water filled cell fluid. The estrogen molecule, being water insoluble, cannot move about within the cell fluid. It must first be activated (hydroxylated by a phase I enzyme) to a cell water soluble hydroxy-estrogen (OH-E), which can then bind to a nuclear estrogen receptor. While bound to a nuclear receptor, the OH-estrogen molecule directs the synthesis of specific proteins from the cell’s DNA template (producing an estrogenic effect). Within hours, the hydroxylated estrogen will be inactivated (methylated, sulfated, reduced, or glucuronidated) by a phase II enzyme. The inactivated, still water soluble estrogen will then be excreted via the liver or kidneys. Estrogen species (bioidentical or pharmacologic) differ greatly in their ability to bind to and stimulate the estrogen receptor(s), and we vary greatly (as a function of genomic and diet/environmental factors) in our ability to hydroxylate (activate) and then to inactivate estrogen molecules. We now have the means to evaluate your ability, as an individual, to metabolize estrogen species.
We can determine your genomic capability to hydroxylate and detoxify estrogens and/or we can measure their “work product” (which is also influenced by diet and environmental factors), the relative levels of hydroxy-estrogens and methyl-estrogens in a urine sample. Putting this information together allows us to provide you HRT with maximum safety and efficacy.
*Orthomolecular = the right hormones, administered the right way, at the right time, in the right patient, with appropriate monitoring of biological effects, and nutritional supplementation to optimize these biological effects.
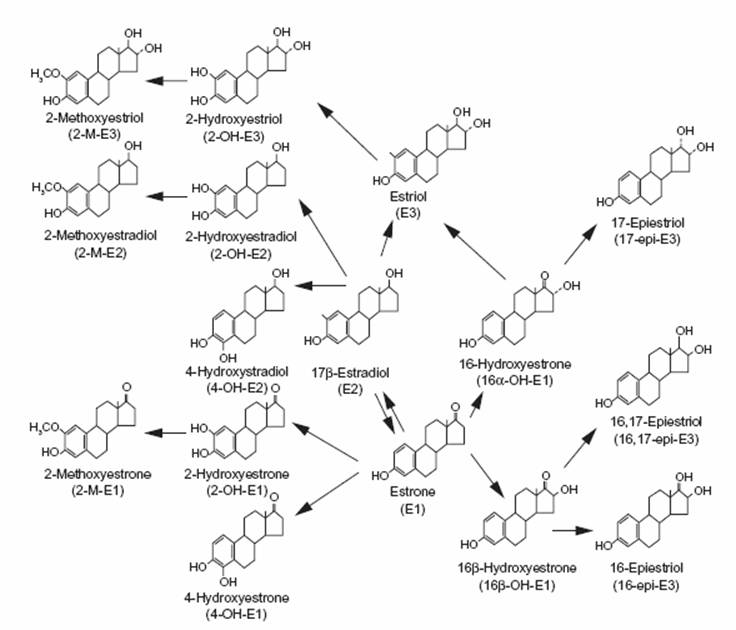
The steroid hormone metabolic pathway is depicted below. Estrogen metabolism, depicted in the lower right triangle, is portrayed in greater detail on page four. Please note that the precursor substance is cholesterol, the raw material from which you generate steroid hormones, bile acids, Vitamin D, and Co-Enzyme Q10. Many of the side effects associated with statin therapy are due to statin induced imbalances in these molecules. We can measure and address these imbalances, allowing you to receive the benefits of statin therapy with fewer side effects (we apply similar analysis to the other prescription meds that you need).
Let’s start with the three basic estrogen species. Estriol (E3) is the dominant estrogen generated during pregnancy. E3 is secreted at much lower levels during reproductive cycling and post-menopause. While cycling, Estradiol (E2) is the dominant estrogen molecule released from the ovaries, while Estrone (E3) of adrenal origin is the quantitatively most important post-menopausal estrogen.
Estrone (E1) Estradiol (E2) Estriol (E3)
Reproductive physiology is all about balance. When Mother Nature presses down on the accelerator, she also begins to tap the breaks. Consider a Woman’s reproductive cycle. During the first two weeks (follicular phase), under the influence of estradiol, the cells lining the uterus (endometrial) and the cells lining the milk ducts begin to proliferate. If conception does not occur, estradiol levels fall, proliferation ceases, the milk ducts return to their resting state, and the endometrial lining sloughs off as menstrual flow. With each cycle of cell proliferation, there is the potential for mistakes to be made in DNA replication (carcinogenic mutations), and thus the greater your lifelong exposure to estradiol (early menarche, late menopause, fewer pregnancies) the greater is your risk of uterine and breast malignancy.
Estrogen effect relates to how tightly a given estrogen molecule binds to the estrogen receptor, for how long, and to its relative binding affinity for the estrogen-alpha (ER-a) vs. the estrogen-beta (ER-b) receptor. As stated above, the greater the number of reproductive cycles, the greater the degree of estradiol mediated bursts of breast and endometrial cell proliferation, and thus the greater potential for genomic error. Mother Nature recognizes this problem, so she created a “braking mechanism” to prevent reproductive cycling from leading to reproductive malignancy. Binding of estradiol to the ER-a receptor leads to breast/endometrial cell proliferation, while binding of estradiol to ER-b blocks proliferation. In addition, Progesterone decreases the binding affinity of estradiol for ER-a while increasing its binding affinity for ER-b.
ER-a is an accelerator, while ER-b and Progesterone serve as brakes.
Mother Nature is very smart; she did not design us to fall ill. Left alone, reproductive cycling does not increase a women’s risk of malignancy. Breast cancer did not occur 100 years ago. It took modern man, introducing genotoxic molecules into the environment, and turning away from anti-cancer foods such as fish oils, flaxseed, and Brassica vegetables, to turn estrogen against us. The chart below estimates binding affinities of the various estrogen species for ER-a and ER-b, as well as the effects of Progesterone species on estrogen binding affinity.
|
|
Relative Binding |
|
|
|
ER-a (accelerator) |
ER-b (brake) |
|
Estrone (E1) |
5 |
1 |
|
Estradiol (E2) |
1 |
1 |
|
Estriol (E3) |
1 |
3 |
|
Premarin (horse estrogens) |
Strong |
Weak |
|
Progesterone |
Decrease |
Increase |
|
Provera (modified progesterone) |
Increase |
Decrease |
Estrone (E1, the dominant post-menopausal estrogen) is a stronger ER-a (accelerator) binder than is Estradiol (E2, the dominant estrogen during reproductive cycling). This explains why breast cancer is more common in post-menopausal vs. pre-menopausal women (other factors are involved). Estriol and Progesterone are high during pregnancy; thus the greater the number of pregnancies, the lower will be a woman’s risk of breast cancer. Premarin, a mixture of horse estrogens, disproportionately binds to ER-a. Thus the use of Premarin (CEE, conjugated equine estrogens) is associated with greater risk vs. that associated with bioidentical estrogen replacement therapy (ERT).

Progesterone Provera (Medroxyprogesterone Acetate)
Provera (Medroxyprogesterone Acetate), a non-human, chemically modified Progesterone (termed Progestin) dramatically increases E1 and E2 binding to ER-a (accelerator) while decreasing their affinity to ER-b (brake). With respect to avoiding asymmetric ER-a > ER-b stimulation, and thus accelerator > brake estrogen action, a thinking person* would prefer the administration of bioidentical estrogens and Progesterone over the use of Premarin and Provera (* in Medical School they lull us to sleep with boring lectures and then sneak in and implant chips in our brains to blunt this process). Because Premarin and Provera are associated with an increased risk of reproductive malignancy and heart disease, we in the medical profession are supposed to tell you that bioidentical ERT and Progesterone will also increase your risk of cancer and heart disease. This is not the case; comparing Premarin/Provera to bioidentical ERT/Progesterone is like comparing whiskey to water. Your other physicians may not agree with me, so allow me to present the science that backs up my position.
Up to the publication of the WHI (Women’s Health Initiative) the standard practice was to recommend Premarin/Provera, to decrease your risk of heart disease and osteoporosis. The WHI looked at event rate in post-menopausal women assigned to placebo therapy, Premarin/Provera, or Premarin alone (if they had undergone hysterectomy). 38/10,000 women in the Premarin/Provera group developed breast cancer vs. 30/10,000 in the placebo group. Thus it was declared that any form of HRT increased cancer risk. Of interest, women assigned to Premarin alone did not experience an increased risk of cancer. This makes sense to you, as you understand that Provera increases Estrogen binding to the accelerator ER-a while decreasing estrogen binding to the ER-b brake; thus it makes sense that Provera would “bring out” or amplify any carcinogenic effects of Premarin. Women assigned to Premarin/Provera also experienced a greater risk of CV events and stroke; thus as a Cardiologist I am expected to tell you that all forms of HRT are bad.
In Europe, physicians and patients made the switch to bioidentical HRT a decade before we in the US did. European studies of Premarin/Provera show the same increased risk as do the US Premarin/Provera studies, but when bioidentical HRT is utilized no risk to slight protection against cancer is demonstrated. The French E3N/EPIC study looked at 80,000 women receiving various forms of HRT over an eight year time frame. Women receiving Provera + Premarin or Provera + Bioidentical HRT were at greater risk for development of cancer (relative risk vs. no HRT of 1.4) while women receiving bioidentical HRT + Progesterone were actually at reduced risk (relative risk vs. no HRT of 0.9). Stated otherwise, including Progesterone in HRT reduces risk of breast cancer (while including Provera dramatically increases cancer risk). This also makes sense to you, as you understand that Progesterone “brakes” the effect of any estrogen species (while Provera “accelerates”). Real Progesterone has an intrinsic anti-estrogenic effect and it encourages binding of estrogen molecules to the ER-b receptor.
Amongst 1083 women attending an infertility clinic, those with low Progesterone levels were 5.4 times more likely to later develop pre-menopausal breast cancer vs. women with normal Progesterone levels. The following study on breast cell proliferation rate supports the above epidemiologic data. Women scheduled for breast reduction surgery were randomized to receive Estradiol, transdermal Progesterone, Estradiol + transdermal Progesterone, or placebo. Breast tissue removed at surgery was then analyzed. Estradiol monotherapy increased breast cell proliferation by 230% (vs. placebo), Progesterone alone decreased proliferation by 400%, while combination therapy had a neutral effect (accelerator + brake = no cellular proliferation).
Comparative studies of Progesterone vs. Provera with respect to symptom control show clear benefits of the former (overall, 65% felt better on Progesterone vs. Provera, with a 30% reduction in sleep problems, 50% in anxiety, 60% in depression, and 30% in somatic symptoms). From the CV perspective, primate and/or human studies have shown that Progesterone dilates arteries, improves lipid parameters, inhibits plaque formation, and has a mild diuretic effect while Provera does just the opposite (as do the other man made Progestins).
The point of the above discussion is to convince you to:
A. Never take Premarin or Provera.
B. Do not fear ovarian hormones (your own of those administered as part of
bioidentical HRT).
C. Think for yourself when medical authorities tell you that any form of HRT
increases risk for heart disease and cancer.
It is not my position that bioidentical HRT carries no risk. It is my position that orthomolecular bioidentical HRT is associated with more benefit than risk. In other words, the good greatly outweigh the bad.
At this point several questions arise:
A. Are there ways to further improve the benefit: risk ratio?
B. Are there individuals who are uniquely susceptible to the downsides of HRT?
C. How can we decrease this risk?
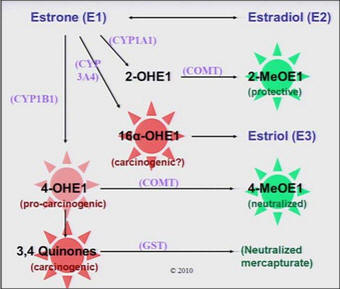
To answer these questions we need to delve deeper into estrogen metabolism. Remember that estrogen molecules (E1, estrone, E2 estradiol, and E3 estriol) cannot dissolve within the cell fluid. They must first be rendered water soluble. Enzymes of the Cytochrome P450 system (known as Phase 1 enzymes) will tack a hydroxyl (-OH) group to E1 or E2 at either its 2, 4, or 16 carbon positions, creating estrogen molecules with widely varying affinity for estrogen receptor binding (later we will cover further metabolism of OH-E2/1 via methylation and reduction; for now we will focus on the pathways on the left side of the graphic below).
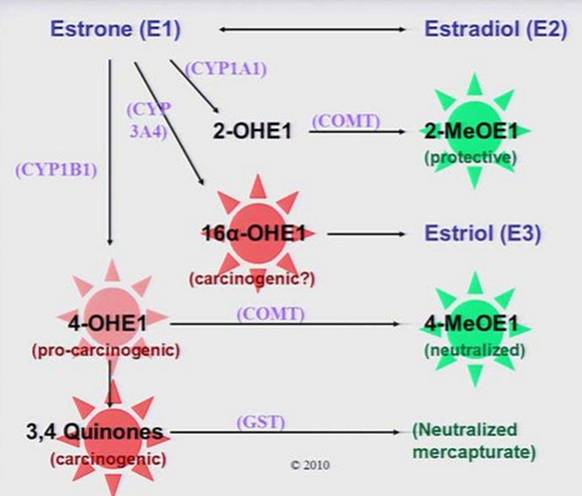
Whether an estrogen (E1 will be depicted in the diagrams but the process applies
to E2 molecules as well) is a strong, weak, or neutral estrogen depends upon
which carbon atom is hydroxylated. Mother Nature did not create
hydroxyestrogens to cause heart disease or cancer
(any more that she created LDL cholesterol to cause arterial disease). Mother
Nature expects these molecules to be present in balance; none are absolutely
good or absolutely bad. However, for purposes of discussion, as we call HDL and
LDL the “good” and “bad” cholesterol molecules, and oxidized LDL "ugly” and
atherogenic, with respect to breast cancer and overall health risk, we will
consider 2-OHE1 to be a “neutral” estrogen, 16-OH to be “bad, carcinogenic”, and
4-OH as “bad, pro-carcinogenic”.


2-OH Estrone 16-OH Estrone
4-OH Estrone
“neutral” “bad,
carcinogenic” “bad, pro-carcinogenic”
When OH-E2 or E1 binds to an estrogen receptor, the OH-E2/1-receptor complex enters the nucleus of the cell and begins to read DNA sequences corresponding to the production of specific proteins. “Estrogenic” protein production lasts as long as the OH-estrogen molecule remains attached to the receptor (this process is also influenced by the enzymes of Phase 2 metabolism, which will be discussed in a later section).
2-OH Estrone and 2-OH Estradiol bind weakly to the estrogen receptor. They basically just sit there and do not initiate “estrogenic” protein production; thus their designation as “neutral estrogens”. 16-OH estrogens species bind more avidly to the estrogen receptor. 16-OH Es are thus “strong estrogens”. While 2-OH and 4-OH Es bind to the estrogen receptors for a few hours, 16-OH Es bind for a day and a half. Thus from the perspective of breast cancer risk, higher levels of 2-OH are preferably to higher levels of 16-OH. These molecules “compete” for binding to the estrogens receptors, and thus your ratio of weak to strong OH-Es determines your risk (amongst other factors) of breast cancer. The majority of OH-Es (fortunately) are 2-OH, with lesser quantities of 16-OH and minimal 4-OH. We can measure the relative levels of 2-OH vs. 16-OH E1 and E2 in urine or serum, and from this data your 2/16 ratio can be calculated. At this point, please ask yourself, do you want a high or low 2/16 ratio with respect to risk for breast cancer? How about in relation to risk of osteoporosis? Now look at the pictures below.


With respect to reproductive organ cancer risk, we want a high 2/16.
|
2-OH Estrone (Estradiol) |
16-OH Estrone (Estradiol) |
|
Weak Estrogen (weak ER-a binding) |
Strong Estrogen (strong ER-a binding) |
|
Protective against cancer |
Promoter of cancer |
|
Antioxidant effect |
Protective against osteoporosis |
|
Protective against atherosclerosis |
|
|
Protective against autoimmune disease |
|
16-OH Es strongly stimulate the ER-a
while 2-OH Es have negligible effect. Thus 16-OH Es are (relatively)
carcinogenic while 2-OH
Es are (relatively) protective. Pre-menopausal women who later develop breast
cancer have 2/16 ratios 30% lower than women who remain cancer free.
The charts below were drawn from two studies of breast cancer risk in relation
to the 2/16 ratio.
Pre-menopausal women with known breast cancer and low 2/16 ratios rarely survive more than 5 years while pre-menopausal women with known breast cancer and normal 2/16 ratios typically survive beyond 10 years.
Post-menopausal women who later develop breast cancer have 2/16 levels 15% below that of women who remain cancer free. Post-menopausal women with known breast cancer and low 2/16 experience a 50% recurrence rate. A low 2/16 ratio is also associated with increased risk of autoimmune disease (lupus, rheumatoid arthritis, and MS) in women, prostate cancer in men (a condition driven by estrogen) and head and neck malignancies. As a general rule, you want a high 2/16. The only down side of a high 2/16 would be an increased risk of osteoporosis (with respect to bone density, the stronger the estrogen effect, the better), but only if your total estradiol levels are low. If estradiol is adequate, then there is no down side, and certainly an anti-malignancy, auto-immune, and atherosclerosis advantage with a high 2/16 (think of a high 2/16 as you would a high HDL: LDL ratio).
4-OHE1 and 4-OHE2 are typically produced in low quantity. 4-OHEs bind more
tightly to ER-a
than does 2-OHEs, and thus are “stronger” estrogens. That’s not the problem.
OH-Es can be oxidized to keto-Es (-OH bond replaced with a =O bond). 4-Keto-Es,
also known as quinones or 3,4 semiquinones, initiate DNA damage and interfere
with DNA repair. These “oxidized”
4-Estrogens cause cancer in the same fashion that “oxidized” LDL cause heart
disease (why I harangue you about taking antioxidants and not just for your
heart). High level 4-Keto-Es are found in breast cancer and to an even greater
extent in men with prostate cancer (basically, everything mentioned above
regarding breast cancer risk applies to men with respect to prostate cancer
risk; 4-Es increase risk). In a latter section, we will learn how to neutralize
4-Keto-Es with glutathione rescue. To summarize, you want a high ratio of 2-OH
to 16-OH Es, you want low levels of 4-OHEs, and above all you do not want your
4-OHEs to be oxidized to 4-Keto-Es.
At this point I’d like to go off subject a bit and tell you that organic pollutants shunt E1/E2 down the 4 and 16-OH pathways and that Cadmium binds tightly to the estrogen receptor and blocks DNA repair (why I also harangue you about metal and organic pollutant detoxification).
 In
the study corresponding
to the charts below and to the left, both ovaries are removed from 28 day old female mice, rendering them
100% estrogen deficient. They are then treated with estradiol (ERT), ICI (which
blocks the estrogen receptor), cadmium, or the combination of cadmium and ICI.
As you can see, cadmium, like estradiol, stimulates uterine and breast
development. As this effect is blocked by ICI, we can conclude that
cadmium is exhibiting a
strong estrogenic effect.
In
the study corresponding
to the charts below and to the left, both ovaries are removed from 28 day old female mice, rendering them
100% estrogen deficient. They are then treated with estradiol (ERT), ICI (which
blocks the estrogen receptor), cadmium, or the combination of cadmium and ICI.
As you can see, cadmium, like estradiol, stimulates uterine and breast
development. As this effect is blocked by ICI, we can conclude that
cadmium is exhibiting a
strong estrogenic effect.
In a similar study, high dose (5 ug/kg) and low dose (0.5 ug/kg, similar to the exposure of American women) cadmium was administered to pregnant rats. Breast development in their teenage (35 days) offspring is greater at both cadmium doses. In American girls, menarche occurs three years earlier now than it did in 1900.
Mistakes are made when our DNA is replicated. Mother Nature understands this, so she gave us an enzyme system to repair post-replication “mismatch”. This enzyme is poisoned by cadmium. Cadmium (and toxins in general), hit us at both ends; they stimulate DNA damage and they inhibit DNA repair. 38/10,000 women in the WHI study taking Premarin/Provera experienced breast cancer vs. 30/10,000 women not taking HRT. Where did breast cancer in these 30/10,000 women comes from? When I was in med school, the teaching was that 1 in 30 women would develop breast cancer. The current risk is 1 in 8 with estimates of 1 in 3 within 10 years (prostate cancer is rising in similar fashion). Metals + organic pollutants + diet/high weight/low exercise + genomic predisposition = disease. This is all about gene-environment interaction. I understand this. I can measure this. I can address this, but first I need you to understand this, as you will be the one to take the corrective actions. This is all up to you.

Now,
back to estrogen metabolism. Our goal is to provide you with ovarian HRT in a
fashion that optimizes the benefits while limiting any down sides, and thus an
important step will be to optimize your 2/16 ratio and minimize 4-OHE
formation. CYPs (cytochrome enzymes) carry out the hydroxylation reactions, and
we vary in the relative strength of our CYP pathways.
CYP 1A1 converts E1 and E2 into the protective 2-OHE, CYP3A4 converts Es into
16-Es, while CYP1B1 generates the equally undesirable 4-OHEs. Many of us harbor
CYPs of varying efficiency, sometimes known as SNIPs. Here the DNA template
codes for an enzyme of increased or decreased efficiency. From a drop of blood
we can look at the integrity of your estrogen hydroxylation and detoxification
pathways (CYPs 1A1, 1B1, 3A4, COMT, and GST). A more practical approach will be
to measure the quantity of estrogen species within a urine sample, and compare
the relative concentrations of the OH-derivatives of E1/E2 (and the ratio of
methylated vs. un-methylated Es, which we will discuss later).
Let’s
first talk about gene – environmental interaction. It irks me when a new
patient tells me that they have a given disease because “they have a family
history” of the disease. This suggests to me that the patient (and their
physicians and our society in general) have blown off their personal
responsibility to optimize health and prevent disease in favor of the easier “I
can’t do anything about it so it’s not my responsibility” approach. Granted,
there are genetic predispositions that fate you to a given disease state, but
nine out of ten genomic predispositions can be attenuated or neutralized if we
take the time to understand the nature of the genomic predisposition and the
factors that aggravate or neutralize it.
Let’s talk about the nature of genomic predisposition. All of us harbor slight
differences (called alleles) in our genomic code for the proteins that make up
our structure and physiology. Substitution of one base pair (such as cytosine
for thymine in the MTHFR gene) will code for enzyme function with varying
degrees of efficiency. These differences are called SNIPS (single nucleotide
interpositions). They are not mutations; they are genomic differences that are
passed down from parent to child. You receive half of your DNA from your Mother
and half from your Father (see Methyl Cycle Genomics on this website for a
more in depth discussion of genomics). I am heterozygous for the NOS (Nitric
Oxide Synthase) down regulation. Thus half of my NOS molecules function
normally, converting Arginine into the vasoprotective molecule Nitric oxide, and
half are sluggish. Thus places me at genomic risk for cardiovascular disease.
As I do not wish to develop cardiovascular disease, I supplement with arginine
and the co-factors that stimulate NOS activity and/or stimulate the reading of
NOS DNA (or if I had known CV disease I might take drugs that favor Nitric Oxide
formation). This “bad” gene will not be my destiny. Rather it is my
gene-environment interaction that determines my destiny (environment here refers
to the conditions within our cells that influence DNA reading and enzymatic
function).
There are genomic predispositions to reproductive organ malignancy that we
cannot (at least not at this time) influence. The BRCA1 and BRCA2 defects
dramatically increase our risk of malignancy (we do not know how so no
strategies to attenuate this risk are available). The BRCA defects are
considered to be of low prevalence but of high penetrance. Only 5% of breast
cancer patients harbor the BRCA genomics, but amongst women born after 1940,
those with the BRCA genes have a life-time breast cancer risk of 85% (women with
breast cancer and BRCA often undergo bilateral full mastectomy when cancer is
detected focally within one breast). Women born before 1940 with BRCA1/2 have a
38% risk of breast cancer. Why the difference? You know the answer – it’s the
environment. A toxic environment, left unaddressed, will bring out the worst in
an adverse genomic predisposition. While we cannot influence the BRCA genomic
predisposition, we can influence the cellular environment and attenuate risk
(that is if we take action) related to the other SNIPs that increase our genomic
risk. Back to our diagram:
 Cytochrome
1A1 (CYP 1A1) converts E1/E2 into 2-OHEs. 2-OHEs bind only weakly to the
estrogen receptor (and can be methylated to the protective methoxy-Es). If you
do not want to develop breast cancer, heart disease, or auto-immune disease, you
want to have a lot of 2-OHE and a high ratio of 2-OH to 16 and 4-OHE.
Conversely, CYP 3A4 and CYP 1B1 takes the same E1 and E2 molecules and convert
them into 16-OH and 4-OHEs, respectively. These Es bind tightly to the estrogen
receptor and cause greater, or more long-lasting estrogenic DNA reading and thus
greater or more long-lasting breast and uterine cell proliferation and thus a
greater risk of malignancy.
Cytochrome
1A1 (CYP 1A1) converts E1/E2 into 2-OHEs. 2-OHEs bind only weakly to the
estrogen receptor (and can be methylated to the protective methoxy-Es). If you
do not want to develop breast cancer, heart disease, or auto-immune disease, you
want to have a lot of 2-OHE and a high ratio of 2-OH to 16 and 4-OHE.
Conversely, CYP 3A4 and CYP 1B1 takes the same E1 and E2 molecules and convert
them into 16-OH and 4-OHEs, respectively. These Es bind tightly to the estrogen
receptor and cause greater, or more long-lasting estrogenic DNA reading and thus
greater or more long-lasting breast and uterine cell proliferation and thus a
greater risk of malignancy.
We can influence these pathways, with lifestyle and nutritional interventions. First we will carry out a urine assessment of E1/E2 levels and the relative levels of 2, 16, and 4-OHEs, then we address any imbalances that you might bear, utilizing measures that promote other aspects of your health (in contrast to drug therapies, that help in one area and often hurt in other areas).
I will start with some summary charts and then we will discuss some of the more important interventions. An up or down arrow refers to a direct effect of a given condition. However, if a condition blocks one pathway, it will indirectly shunt E1/E2 metabolism down the other pathways, and vice versa.
|
Effect on Estrone/Estradiol Hydroxylation by CYPs |
|||
|
Parameter |
2-OH |
16-OH |
4-OH |
|
CYP 1A1 |
|
|
|
|
CYP 3A4 |
|
|
|
|
CYP 1B1 |
|
|
|
|
CYP 1A1 Defect |
¯ |
|
|
|
CYP 3A4 Defect |
|
|
|
|
CYP 1B1 Defect |
|
|
|
|
Smoking |
|
|
|
|
Overweight |
¯ |
|
|
|
Exercise |
|
¯ |
¯ |
|
Low Weight |
|
¯ |
¯ |
|
Thyroid Hormone |
|
¯ |
|
|
Hi Protein vs. Hi Carbs |
|
|
|
|
Omega-3s vs. 6s |
|
¯ |
|
|
Inflammation |
|
|
|
|
Cruciferous Veges |
|
|
|
|
I-3-C and/or DIM |
|
|
¯ |
|
Soy Isoflavones |
|
¯ |
¯ |
|
Flax Seed |
|
¯ |
|
|
Organic Pollutants |
|
|
|
|
Premarin |
|
|
|
|
DHEA |
|
¯ |
|
|
Bioflavonoids |
|
¯ |
|
|
Vitamin D |
|
|
|
CYP1A1 hydroxylates E1/E2 at the 2 position. The CYP 1A1 defect is a down
regulation, compromising your ability to 2-hydroxylate. If you are heterozygous
(+/-, one good gene and bad gene), you will have trouble with 2-hydroxylation
and if you are homozygous (+/+) you will have great difficulty. Supplements
designed to up regulate 2-hydroxylation via CYP 1A1 will not work well for you,
and your risk of reproductive malignancy will be increased.
African-American
women with the CYP1A1 Msp-1 polymorphism have a 9.7 fold increased risk of
breast cancer. While baseline 2/16 levels are comparable to those of women with
normal 1A1 function (wild type), 2-hydroxylation and the 2/16 ratio increase
less in response to Indole-3-Carbinol (I3C) supplementation. The CYP3A4 and 1B1
polymorphisms code for up regulated (more rapid than wild type) hydroxylation of
E1/E2 down the 16 or 4-OH pathways, respectively. If you harbor these alleles
you will be at increased risk for reproductive malignancy, and while risk
associated with these alleles is typically studied one allele at a time, it is
reasonable to state that the greater the number of undesirable polymorphisms you
possess, the greater will be your risk.
If you harbor these hydroxylation defects (and we can test for them), you are
not doomed to reproductive malignancy, but your are at increased risk, and
paying attention to the other factors that influence estrogen metabolism becomes
even more important. Genes are not your fate. It is knowledge and the personal
strength to use knowledge that determines your fate. Stated otherwise, genes do
not doom us. It is the lack of knowledge and the lack of personal strength to
use this knowledge that allows genomic predisposition to bring out the worst in
our health.
We’ve talked about the hydroxylation pathways and the genomic conditions that influence their function. Now let’s talk about the lifestyle and nutritional factors that we can control.
Smoking induces CYP1A1. If you smoke, you will make more of the enzyme that converts E1/E2 down the 2-OH pathway. In this particular function, smoking thus decreases your risk of breast cancer, as the more “neutral” 2-OHE you make, the less “genotoxic” or “pro-genotoxic 16-OH and 4-OHE will be generated. Your 2/16 and 2/4 ratios will rise. Please understand that the 2/16 benefits of smoking are far outweighed by the cadmium and free radical burden associated with smoking, but feel free to misquote me a little and tell your teen age daughters and granddaughters that smoking might decrease breast size (more 2-OH and less 16-OH leads to less breast tissue proliferation).
 Overweight
increases your cancer risk, especially your reproductive organ cancer risk.
Overweight women make less 2-OH and relatively more 16-OH and 4-OH Es than do
trim women. A molecule that can be eluted (probably a cytokine) form visceral
fat directly inhibits the action of CYP1A1. Conversely, trim women have a more
protective ratio, and weight loss as an intervention will dramatically improve
(increase) your 2/16 ratio. Exercise does the same thing. Elite female
marathon runners are thin, bear small breasts, and stop menstruating. They are
making so much 2-OH E2 (and E1) that there is not enough 16-OHE2 available for
normal cycling. This makes sense. Primitive woman did not run marathons, but
she would set out on long treks across the wilderness in search of food. This
was not the time to conceive, or to waste energy in reproductive cycling. Thus
in this situation of prolonged exertion/limited availability of food, Mother
Nature alters the way a woman reads her DNA in a fashion that optimizes her
ability to survive in her current environment. With a reduction in exercise or
weight regain, E2 shunting down the 2-OH pathway slows down, more 16-OH can be
made, and reproductive cycling will resume (the famine is over; food is
plentiful, so now it is OK to conceive).
Overweight
increases your cancer risk, especially your reproductive organ cancer risk.
Overweight women make less 2-OH and relatively more 16-OH and 4-OH Es than do
trim women. A molecule that can be eluted (probably a cytokine) form visceral
fat directly inhibits the action of CYP1A1. Conversely, trim women have a more
protective ratio, and weight loss as an intervention will dramatically improve
(increase) your 2/16 ratio. Exercise does the same thing. Elite female
marathon runners are thin, bear small breasts, and stop menstruating. They are
making so much 2-OH E2 (and E1) that there is not enough 16-OHE2 available for
normal cycling. This makes sense. Primitive woman did not run marathons, but
she would set out on long treks across the wilderness in search of food. This
was not the time to conceive, or to waste energy in reproductive cycling. Thus
in this situation of prolonged exertion/limited availability of food, Mother
Nature alters the way a woman reads her DNA in a fashion that optimizes her
ability to survive in her current environment. With a reduction in exercise or
weight regain, E2 shunting down the 2-OH pathway slows down, more 16-OH can be
made, and reproductive cycling will resume (the famine is over; food is
plentiful, so now it is OK to conceive).
Cruciferous vegetables, I3C, and DIM: Cruciferous, also referred to as Brassica, vegetables, include cabbage, broccoli, turnip, mustard, kale, rutabaga, Brussels’ sprouts, cauliflower, kohlrabi, and collards. Along with other health promoting and detoxifying substances (such as sulflorphane), cruciferous vegetables contain Indole-3-carbinole (I3C) which undergoes dimmerization within the acid environment of the stomach to yield Diindolylmethane (DIM) a potent anti-inflammatory and anti-cancer nutritional.
Estradiol
I3C DIM
I3C and DIM share a structural similarity to E1/E2, and by this means interact with the pathways of E1/E2 metabolism. Cruciferous vegetables provide multiple health promoting effects, but within this discussion we will present both I3C and DIM as strong CYP1A1 pathway stimulators and CYP3A4 inhibitors. Stated otherwise, these agents will increase 2-OH and 2/16 and decrease 16-OH E formation. In animal models, I3C/DIM have strong anti-cancer effects. In humans, if the CYP1A1 pathway is genomically intact, I3C or DIM at 200 mg twice a day should double 2-OH E production.
The chart to the left shows the effect of 400 mg/day of I3C in a healthy individual.
Cervical Intraepithelial Neoplasia (CIN) is a precancerous condition of the cervix due to persistent infection with human papilloma virus (HPV). HPV thrives in a high 16-OH E environment. So what happens when women with CIN are treated with I3C? They improve. HPV is also associated with laryngeal papillomatosis in kids. Here the virus induces growths on the vocal cords that must be scraped off surgically. Treatment with I3C reduces disease severity and decrease the need for surgical intervention.
Flaxseed contains omega-3 fatty acids, which provide an anti-inflammatory
effect, but with respect to estrogen metabolism we are more interested in the
lignans found in freshly ground flaxseed (thus we want the flax seed, not just
the flax seed oil). Flaxseed derived lignans inhibit
the bacterial enzyme beta-glucoronidase.
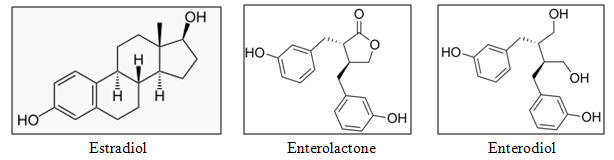
One pathway through which OH-Es are inactivated is to bind them with glucoronic acid, which facilitates their excretion into the GI tract. If bacterial beta-glucoronidase breaks the E1/E2-glucoronate bond, then the E1/E2 molecule can be reabsorbed back into the circulation. Two flaxseed lignans, Enterolactone and Enterodiol, share structural similarity with E1/E2, and like I3C/DIM, will favorably affect E1/E2 metabolism. In one study, 10 grams/day of ground flaxseed baked into a muffin increased 2-OH E levels by 34% and the 2:16 ratio by 21%.
Isoflavones, such as Genistein and Daidzein are found in beans, legumes, soy, lentils, and other plant-based foods. Soy is particularly rich in isoflavone content.
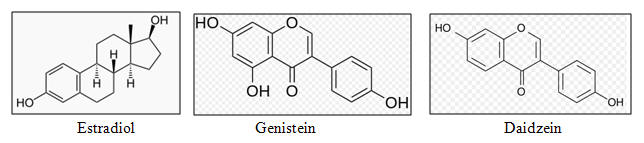
Isoflavones up regulate 2-hydroxylation and favorably effect the 2/16 and 2/4 ratios. In one study, the administration of 158 mg/day of isoflavones lead to a 50% increase is 2-OH E1 formation, with concomitant decreases in 16 and 4-OHE1, such that the 2/16 ratio rose from 2.0 to 2.6. Traditional Asian diets may be protective due to their high content of soy products, and this is associated with reduced risk of breast, prostate, and endometrial cancers.
Organic Pollutants, such as benzene, toluene, parabens, and phthalates, are fat soluble toxins that Mother Nature did not prepare us for. We do not do a good job of detoxifying these agents, such that they bioaccumulate within visceral fat and nervous tissues (thus they are termed POPS – persistent organic pollutants). Without intervention (far infrared sauna, foot bath therapy, or supplements designed to up regulate liver phase I and phase II detox), the only dependable means available to rapidly lower your own POP burden is to have a baby and then breast feed your child. Thus you see the problem that industrialized societies face. These agents, especially phthalates (the stuff that renders plastic soft and malleable) lower metabolic rate in visceral fat and disrupt the insulin receptor, predisposing you to weight gain. They directly stimulate the estrogen receptor and shunt E1/E2 metabolism down the 16-OH pathway. This biochemical disaster is playing a role in the epidemic nature of obesity, diabetes, and reproductive organ malignancy that is occurring in the industrialized world. Serum phthalate levels correlate with premature menarche in girls. In animal models, phthalate administration does not affect E1/E2 2-hydroxylation by CYP1A1, but it increases 16-hydroxylation by 3A4 and of greater concern 4-hydroxylation by 1B1.
In later sections we will cover phase II E1/E2 metabolism, and means of
obtaining bioidentical HRT, but at this point, what can we do the information
already discussed?
First, if you chose to receive HRT, do not take Premarin, Provera, or any
man-altered molecule. Instead take bioidentical estradiol, progesterone, and
testosterone, administered in a physiologic fashion (do not take any form of
estrogen HRT orally, even bioidentical; it is the first pass metabolism through
the liver that leads to the increased risk of clot formation identified in the
Premarin/Provera studies).
Second, if you are post-menopausal or still cycling, whether you are or are not
taking HRT, whether you are female or male, undergo an assessment of estrogen
metabolism. This involves a first morning void or 24 hour urine assessment of
estrogen hydroxylation and methylation products (fully covered by Medicare, with
a co-pay of
»
$144 if you have commercial insurance). If your 2/16 or 2/4 ratios are low,
then we can and should intervene with lifestyle measures such as increased
exercise and weight loss, and/or supplements such as fish oil, flax seed, soy
isoflavones, and vitamin D. Brassica vegetables, three meals per day are ideal,
but if that is not possible you can supplement with either I3C or DIM. If you
are hypothyroid we will correct that condition, and we can evaluate you for
organic pollutant overload (US BioTek study – seven major POPs for $126) and
then help you rid yourselves of these toxins (and later on we can look for and
address heavy metal overload). If you are post-menopausal and not on HRT, our
goal will be a 2/16 between 2 and 3, with a physiologic 4-OH level. If you are
still cycling or on HRT, such that E1/E2 levels are in the physiologic range,
then we can aim for a higher 2/16 (remember, the only down side of a high 2/16
would be an increased risk of osteoporosis if 2/16 is high and Estradiol is
low).
There really is no reason not to carry out this analysis in all men and women, to decrease our risk of reproductive malignancy and auto-immune disease. None of these measures can do anything other than improve other aspects of our health, and none of these measures are particularly expensive, especially when you consider the consequences of not taking these steps.
Now
let’s move on to the second phase of estrogen metabolism. Back to our chart:
As previously stated, 2-OHEs are neutral. They bind to the estrogen receptor
and just sit there, but as 2-OHEs “crowd out” the 16-OH and 4-OH Es, the more
2-OHEs present, the lower will be your risk.
Now, if 2-OH E1 or 2-OH E2 is methylated by COMT, a key enzyme of phase II
metabolism, 2-methoxyEs are created. These molecules provide powerful
anti-cancer, anti-heart disease, and anti-autoimmune disease protection.
Conversely, 4-OHEs can be oxidized into carcinogenic 4-Keto-Es (3,4 Quinones in
the chart). However, 4-OHEs methylated by COMT into 4-methoxyEs are rendered
inactive. The negative effects of E1 and E2 trafficking down the 1B1 pathway
will thus be attenuated. We want to create 2-methoxy and 4-methoxyEs. We
create these molecules by supplementing with agents that lower Homocysteine,
agents that we also advise to reduce your risk of heart disease, depression, and
neurodegenerative disease, and to reduce the risk of spina bifida.
Phase I enzymes activate molecules, endogenous and toxic. Phase II enzymes tack
on a chaperone (methyl, sulfate, glucoronic acid, etc.), rendering the activated
molecules water soluble and thus easier to excrete (our protocol for organ
pollutant detoxification includes supplements that stimulate and support both
phase I and phase II processes). COMT (catachol-O-methyl transferase) tacks a
methyl group (CH3, a carbon with three hydrogen atoms attached) to a OH-E to
form a methoxy-E. In like fashion, it tacks on a methyl group to inactivate
adrenalin, caffeine, and other endogenous and exogenous substances. Proper
metabolism depends upon proper methylation, which depends on proper function of
the Methyl Cycle enzymes. This concept is discussed in gene by gene detail on
the heartfixer.com website (the critical importance of Methyl Cycle genomics was
brought to our attention by Dr. Amy Yasko
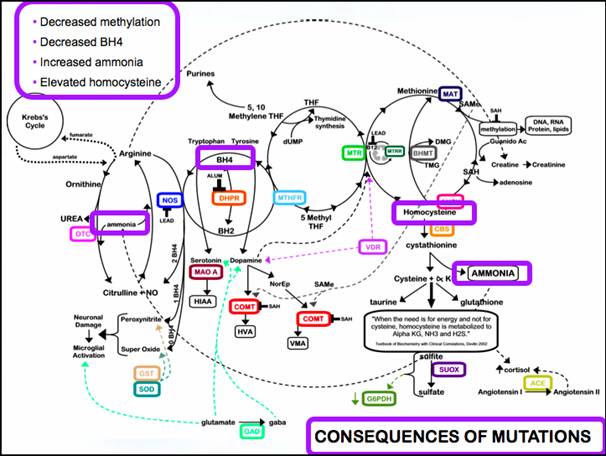
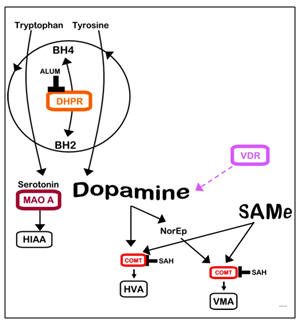
and these two charts come from her book, Genetic Bypass; her website is
holisticheal.com), but basically involves the shuttling of methyl groups from
methyl-folate and methyl-B12 to methionine to form S-adenosyl methionine (SAMe),
the universal methyl donor). SAMe donates the methyl group that is used by COMT
to methylate OH-Es, adrenalin, caffeine, etc. Many factors can disrupt the
Methyl Cycle and thus our ability to methylate OH-Es; these include genomic
polymorphisms in the Methyl Cycle enzymes, B-vitamin deficiency due to commonly
prescribed prescription agents, and environmental toxins, particularly metals
such as mercury, lead, and aluminum (you are now caffeine sensitive but in your
20s you had no trouble with caffeine; your DNA hasn’t changed but you have
accumulated enough toxicity to shut down methylation). While COMT had many
important roles, our interest here is in optimizing COMT function to promote
beneficial 2-OHE methylation and neutralizing 4-OHE methylation. How do we
achieve this (while supporting other beneficial aspects of our biochemistry)?
If COMT is functioning normally, all we have to do is to supplement with SAMe
200 mg/day. SAMe provides the methyl group that COMT uses to methylate OH-Es.
Better yet, we could stimulate endogenous production of SAMe by supplementing
with B vitamins. As many of us, on a genomic basis (and many more of us due to
toxicity), harbor sluggish methyl cycle enzyme systems, supplementing with pre-methylated
B vitamins (methyl-folate and methyl-B12) will be more efficient. Other “methyl
donating” agents such as trimethylglycine (TMG), theanine, melatonin, and
turmeric may be of value here. Some of us (20% in the US) harbor a
dysfunctional COMT genotype. If we are heterozygous for COMT (+/-), our ability
to methylate OH-Es will be compromised. If we are homozygous (+/+), our
methylating ability will be only 20% of normal. Methyl donors will not be
effective and at high dose might compromise other aspects of our physiology (the
“dammed up” methyl groups will overload other pathways). In this situation, we
will not push methylation; instead we will focus on optimizing your (hopefully)
intact phase I pathways and in optimizing the “rescue” reduction (antioxidant)
pathway (discussed later). We can evaluate your COMT genotype within both the
Yasko Methyl Cycle and Genova Labs Estrogenomic or DetoxiGenomic panels. In all
individuals, we wish to optimize COMT and methylating function with adequate B
vitamin intake and by lowering our toxic burdens (with reference to COMT,
mercury is probably the most important toxin).
|
Key Supplements to Support Methylation |
||
|
Methyl-Folate |
Methyl-B12 |
SAMe |
|
Magnesium |
Methionine |
TMG (Trimethylglycine) |
16-OHEs are powerful estrogens. However, they can be “reduced” via the addition of another OH group to form the tri-hydroxy estrogen molecule, estriol. As discussed (several biochemistry classes ago), this “ultra weak” estrogen binds the ER-b (brake) three times more avidly than the ER-a (accelerator) receptor. How do we encourage conversion of genotoxic 16-OHE into protective estriol? We optimize our antioxidant status. We take in antioxidant and bioflavonoid rich fruits and vegetables, supplement to make up for any deficiency that nutritional testing might uncover, and we remove from our body pro-oxidant organic pollutants and metals. Have you heard me talk like this before? Antioxidant protection is important, and from the perspective of cancer prevention it is particular important if you bear the down regulations for CYP1A1 and COMT and/or the up regulations for CYPs 3A4 or 1B1. Genes are not our fate; if we understand our genomic predispositions we can always find ways of bypassing our blocks while maximizing our open pathways. Most likely you understand the concept of an antioxidant “defense team”; if not please review our DVD presentation Antioxidants – The Cornerstone of Preventive Cardiology. Antioxidants which might specifically relate to 16-OHE reduction include green tea extract (ECGC) and Resveratrol.
Glutathione Rescue – Let’s say that you have an unfavorable genotype (CYP1A1 and COMT down regulations and CYP1B1 and 3A4 up regulations). Post-menopause, with the loss of ovarian hormone support you’ve put on weight; you hurt your back so you can’t exercise like you used to, and you don’t take antioxidants as your other doctors told you that antioxidants produce only “expensive urine”. Your 2/16 and 2/4 ratios will be low, you can’t neutralize 16-OHEs in to protective estriol, and you can’t optimize the 2-OHEs that you can still make (at low levels) into the protective 2-methoxyEs. You are making large amounts of 4-OHEs and you are oxidizing then into the mutagenic 4-ketoEs. These molecules occupy davits in DNA strands, block DNA repair, and result in malignant transformation. Things are not looking too good for you, but Mother Nature has one more rescue mechanism in her arsenal. An enzyme known as GST (Glutathione-S-Transferase) can bind a glutathione molecule to a 4-ketoE, converting it to a harmless molecule known as a mercapturate. GST acts like HDL. HDL reduces oxidized LDL (which initiates atherosclerosis) back to harmless LDL cholesterol (cell food - the raw material from which we generate steroid hormones). Thus we want a healthy and functional GST system. GST efficacy is under genomic and nutritional control. Some of us harbor variants whereby glutathione rescue is compromised, placing us at risk for malignancy (and many other disease states as glutathione is our most important intracellular antioxidant and detoxifier; we can assess your GST status within the Genova Labs DNA studies). The greater our level of free radical oxidative stress, the more toxic metals and organ pollutants (especially mercury) we bear, the lower will be our glutathione pools and GST functionality. To optimize glutathione rescue, as stated above with respect to reducing 16-OHEs to estriol and optimizing health in general, supplement with antioxidants and remove from your body the toxic molecules that Mother Nature did not intend you to bear.
|
Key Supplements to Optimize Glutathione Physiology |
|||
|
Selenium 200 mcg |
Lipoic Acid 1-300 mg |
N-Acetyl Cysteine 500 mg |
Glycine 1000mg |
We’ve covered the biochemistry of estrogen metabolism. You know not to take man-altered hormones, and you are now acquainted with the means to optimize how your body will hydroxylate, methylate, and reduce estrogen molecules. A healthy diet and lifestyle will go a long way, and we can examine the integrity of your estrogen metabolic pathways with the above described (and relatively low cost) urine study. If you wish we can evaluate your genomic status with the (relatively more expensive) Genova Labs DNA study. This makes sense for all of us. These principles apply to pre and post-menopausal women and to men with respect to prostate cancer risk.
If you are interested in orthomolecular HRT, and you are peri-menopausal, our first step will be to carry out a 28 day hormone assessment. Here we measure salivary estradiol, progesterone, and testosterone, every three days over an entire cycle. This way we can determine which hormones you need, and at which time within your cycle. We may also wish to look for abnormalities in thyroid and adrenal function, and to look for organic pollutant and metal toxicity.
If you are post-menopausal with obvious deficiency symptoms, simple baseline blood studies will be carried out and HRT initiated. As a rule, we will not use any form of oral estrogen. Oral estrogens increase risk for clot formation; this has not been described for non-oral therapy. If we are worried about a genomic clotting risk Genova Labs has a corresponding DNA evaluation (Factor 2, Factor 5 Leiden, PAI-1, and glycoprotein3a).
Bioidentical estrogen and testosterone may be administered topically, in a lipophilic (fat soluble) cream or gel, via the sublingual route, or in the form of subcutaneous pellets that are placed every six months. The latter route is preferred as it leads to steadier and more predictable blood levels. I was trained in this technique by Dr. Gino Tutera (see sottopelletherapy.com website). If we use a topical preparation, we cannot use blood levels to monitor hormone efficacy and dosing. Hormones administered via the skin bind tightly to red cells and are underrepresented in the serum. Thus if we use serum levels to monitor dosing we could easily give you more hormone than you need. When this occurs, the hormone receptors down regulate, and you feel as if you are not getting enough hormone, so we might give you a higher dose, aggravating the situation and increasing your risk for adverse reactions. If we administer estrogens and testosterone via a topical cream, we will monitor levels from capillary blood (blood spot testing), saliva, or urine. With pellet HRT we can use blood levels (which your insurance is far more likely to cover). We prefer oral over topical or sublingual progesterone. Oral progesterone is metabolized in the liver to allopregnanolone, and agent with calming and sedative effects; thus you take oral progesterone (compounded or as the prescription agent Prometrium) in the late evening.
We pick a starting dose in relation to your age and symptomatic status, and then adjust the dose in relation to your levels and symptomatic response. After we have arrived at a stable dose, then a 24 hour urine for estrogen hydroxylation and methylation products (and from the same study we can also quantitate E1, E2, E3, testosterone, and progesterone), and then apply the principles discussed above to optimize your 2/16 and 2/4 ratios, convert 2-OH and 4-OHEs into their methoxy derivatives, reduce 16-Es to estriol, and convert any 4-keto-Es in to non-toxic mercapturates. In this fashion we can optimize your symptomatic status and overall health while minimizing the risk of any adverse hormone related effects. As we aren’t perfect, it is important that you undergo pelvic and breast exams on a yearly basis, along with breast imaging (mammogram, thermogram, or MRI) as recommended by your primary physician or OB-Gyn specialist. I can’t do this as I don’t know how. I am a cardiologist who understands human biology and biochemistry as taught within the Fellowship program in Anti-Ageing and Regenerative Medicine (faafm.com – check out the faculty roster; scroll down to the Rs) co-sponsored by the American Academy of Anti-Ageing Medicine and the University of South Florida Medical School (the ABAARM behind my name means that I am certified by the American Board of Anti-Ageing and Regenerative Medicine - I have completed the requirements as an Advanced Fellow). Rely on me for your biochemistry, but work with your other practitioners regarding malignancy screening and other aspects of reproductive health.
James C. Roberts MD FACC
FAARFM
9/16/2012