Return to CHC Home Page Return to Treatments Available
Return to Diagnostic Studies Return to Medical Topics Home Page
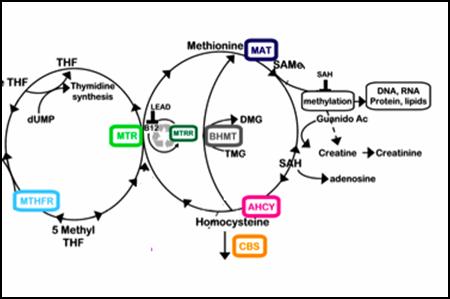
Methyl Cycle NutriGenomics
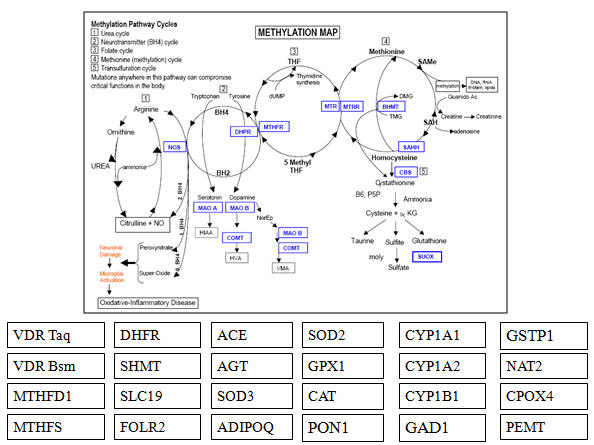
The Methyl Cycle is the backbone of our physiology. It's functional status determines our resistance or susceptibility to environmental toxins and microbes. This is a confusing array of biochemistry, but suffice it to say, a defect at any one point in these interlocking cycles will inevitably affect the remaining pathways, and your overall health will then suffer. Methyl Cycle abnormalities explain why you are sick from environmental toxins while the guy next door is just fine, why you are autistic while your fraternal twin brother is not. While we cannot change your DNA, if we know your weak links we can create "nutritional workarounds" - we can supplement alternative pathways or withhold from your diet molecules that you cannot handle. If we do not address the Methyl Cycle abnormalities that underlie unexplained or chronic illness - well then the illnesses will remain chronic and unexplained, because it is the Methyl Cycle Abnormalities that predisposed you to ill health. As antioxidant and detoxification genomic testing is now low in cost, we are extending our attention to variant function in these important systems as well. the more we know about your genomic weaknesses, the easier it is for you to overcome them.
Methyl Cycle Genomic Analysis and Supplementation Overview
Getting Started - How to Obtain Your Genomic Profile
Individualized Methyl Cycle, Antioxidant, and Detoxification Genomic Analysis
Methyl Cycle Presentation Power Point Slides
CBS: Cystathionine Beta Synthase - Explanation and Generic Plan of Action
CBS: Cystathione Beta Synthase - Old Explanation
MTHFR C677T and A1298C - Explanation and Generic Plans of Action
MTHFR C677T: 5,10-Methylenetetrahydrofolate Reductase (Þ 5-Methyl-Folate) More In-Depth Explanation
SHMT: Serine Hydroxy Methyl Transferase
MTRR: Methionine Synthase Reductase
BHMT: Betaine-Homocysteine Methyltransferase
COMT: Catechol–O–Methyl Transferase
VDR Taq: Vitamin D Receptor Taq Abnormality
MTHFR A1298C: 5,10-Methylene Tetrahydrofolate Reductase (Þ BH4)
Methyl Thieves and SAMe Stealers
ACE: Angiotensin Converting Enzyme
Glutamate – GABA Imbalance Þ Excitotoxicity
MAO A, ACAT, AHCY, and VDR Fok
Appendix I: Foods High in Tyrosine or Tryptophan
Appendix II: Foods High in Sulfur
Appendix III: Foods High in Excitotoxins
Appendix IV: Elevated Urine Sulfate - What Do You Do Next?
Appendix V: General Recommendations Based Upon the Sulfate Value
Appendix VI: Methyl Cycle Recipes
Nurtigenomic Supplements and Supplies
Ordering Supplements from Websites
What You Can and Cannot Expect From Us
Sample Report - Child with Neurodevelopmental Challenges
Sample Report - Adult with Chemical Sensitivity
Sample Report - Adult with Fatigue and Chemical Sensitivity
Sample Report - Adult with Atherosclerosis
Methyl Cycle Genomic Analysis and Supplementation
Understanding how to incorporate the science of Methyl Cycle Genomics in to your
treatment program, and how best to monitor your individual response, will be a
challenge to both of us. If we accept this
challenge, and spend time, energy, and resources in dealing with your Methyl
Cycle Abnormalities, then you can take strides forward in improving your
health. If we do not – well, most of you are undergoing Methyl Cycle testing
because you have a health problem that makes little sense; you have seen
multiple doctors and you are not getting better – if we do not address your
Methyl Cycle abnormalities then we cannot expect that you will get better –
because it is the
Methyl Cycle Abnormality that predisposed you to ill health.
What is a Methyl Cycle Abnormality? The chart above describes mutations, scientifically a correct descriptor, but not a good common language description of your condition. You do not have a “mutation”, a one-time genetic accident that occurred during your embryonic development. Methyl Cycle Abnormalities are not disease specific or smoking gun genetic defects. Yes, there are specific genetic abnormalities that code for Sickle Cell Anemia, Huntington’s Chorea, or Phenylketonuria, and if you are born with these genotypes (referring to one’s genetic code), then we can be 100% certain that you will develop these disease states (the phenotype, or expression of the genetic code). There is a great deal or dread and anxiety regarding testing for these genes. After all, if you can’t do anything to prevent the phenotype, why even look for the genotype?
Methyl Cycle Defects are different. None code for a specific disease state, but all play a role in predisposing you to disease in general. The more Methyl Cycle Defects present in your genotype, the greater is your susceptibility to toxicity and infection, and the greater will be your risk for these (usually) age-related degenerative disease states that plaque our society today. These disease states are usually age-related (but are occurring in you earlier than in others) because it takes time for toxicity to build up within you, to overcome the still intact defense systems that are trying to defend your physiology. On the other hand, a little bit of toxicity during a vulnerable time period can do a lot of damage to an individual with impaired Methyl Cycle defenses. The frequency of Methyl Cycle Defects in autistic kids will likely be 100% - a little bit of Mercury in a genetically defenseless kid will damage a developing brain. Their parents and grandparents harbored these genes (likely in lower concentration) but when they were born our uterine and early life environment was toxin free. Their brains had the chance to develop normally. Exposing them to toxicity now isn’t good for them, but their brains did have the chance to develop normally, so they do not develop “adult onset autism”. But individuals harboring Methyl Cycle Defects are going to get sick, before their time, likely with conditions that make little sense such as Fibromyalgia, Chronic Fatigue, Multiple Chemical Sensitivity, or they will present early in life with what used to be diseases seen only in “old people”: - coronary disease, cardiomyopathy, Parkinson’s disease, and dementia.
I’ve looked at disease as a combination of lifestyle, environment, and heredity. Yes, if you smoke, you will eventually experience lung disease. If you are exposed to lead then it will eventually build up in your body and cause hypertension and kidney disease. But some people smoke and get lung disease at an early age, some only at old age, and some seem to be able to puff away into their 80s. We are all exposed to multiple toxins, we all live in the same general environment, but only some of us get heart disease and cancer – why? If toxicity is so bad, then why don’t all of us have toxicity associated cancer? Well, we’re on our way, but some of us can live within this toxic environment unscathed. How can one boy be autistic while his fraternal twin is normal - same uterine environment, same maternal diet, same vaccinations – but different genotypes. It is our genotype, specifically the status of the genes making up our Methyl Cycle that render us more or less susceptible to environmental influences (toxins and microbes).
The term “methyl group” refers to CH3, one carbon atom attached to three hydrogens. The enzymes of the Methyl Cycle add or subtract a methyl group from another molecule to open or close biochemical pathways, to open our DNA when it should be read, or to close it when it would not be in our best interest to decode a specific gene. We need methyl groups to silence viral RNA, to defend against other microbes, and to defend against environmental toxins. Optimal methylation is thus more important today than it was in years past, when the environment was less toxic. Individuals with Methyl Cycle Defects are the canaries of our society. Toxins will hurt all of us eventually but those of us with Methyl Cycle Defects will be the first to go down.
I am now looking at disease as a combination of lifestyle, environment, and Methyl Cycle Genomic Defects.
Your packet contains your genotype. It is up to you to adjust your diet, and it is up to me to change your treatment program, in order to optimize your phenotype (your health status – the expression of your genotype). We can’t change your genotype, but we can optimize its expression. We can eliminate from your diet and treatment program substances that you cannot handle, and we can supplement you with substances that you cannot make on your own. We can bridge gaps in your metabolic software and shore up your weak links – now that we know what your weak links are. This will be a lot of work and involve a not insignificant out-of-pocket expense, and likely a major change in your diet. This may irritate you. You may initially be frustrated and mad. If you want to be mad, you can be mad at me – but don’t go after me on a busy day – I am COMT -/- and VDR Taq +/+; thus if you stress me out too much I will be susceptible to a fall off in dopamine, serotonin, and norepinephrine, so I won’t think so well (a little Methyl Cycle humor). Please do not take out your frustration on my staff. If you are really angry you can complain to your parents, Charles Darwin, or God – a better idea will be to accept and understand this challenge and get to work addressing it. Along with your genotype report, your packet will contain Dr. Yasko’s general recommendations (which focuses on kids with Autism), my analysis of your genotype with specific recommendations for diet change, nutritional supplementation, and follow-up testing. Information regarding sulfur avoidance (critical for CBS and SUOX genotypes) and food excitotoxin avoidance (useful for all of us) will be enclosed, along with a supplement check list and information regarding how to obtain these supplements on line or at the office.
90% of you will have an abnormality in the trans-sulfuration pathway (CBS and/or SUOX). Sulfites and Chronic Disease, by Rick Williams (available at the office or you can go to www.readingtarget.com/nosulfites) contains a great deal of information regarding the sulfite/sulfate content of common foods and pharmaceuticals. Read and research on your own, particularly with respect to diet, and report back to us on what worked and what didn’t work with respect to lowering your sulfate/sulfite levels – with feedback from you we can improve our general recommendations.
Regarding our terminology: homozygous, heterozygous, (+/+), (+/-), and alleles, let’s start with a review of genetics and gene distribution - we can use me as an example. I am homozygous (+/+) for MTHFR C677T. C (cytosine) has been replaced by T (thymidine) in the 677th nucleotide position in my genes for the MTHFR enzyme. C codes for the amino acid alanine and T for the amino acid valine. Thus I have a valine where I should have an alanine within the amino acid structure of 100% of my MTHFR enzymes. This enzyme will not work well. It will not efficiently convert folic acid in to one of its active forms, 5-methyl folate. I can take all the folic acid I want, but I cannot use it. With respect to this biochemical step, folic acid will actually be toxic to me, as it will crowd out the sparse methyl-folate present in my diet. If my diet is confined only to folic acid, I am going to have trouble metabolizing homocysteine, and I am going to have trouble carrying out many other critical biochemical steps. I will be at risk for premature cardiovascular and neurological disease. If on the other hand I supplement with 5-methyl folic acid, I will have bypassed this genetic block, my biochemistry will revert to normal, and my increased individual risk associated with the C677T abnormality will be 100% resolved. I also realize that 100% of my kids will be at least heterozygous (+/-) for the C677T allele (if they are not then we will have to look closely at the mailman), and if my wife is heterozygous (+/-) or homozygous (+/+) for the C677T allele, then they too may be homozygous (+/+). “Allele” refers to a variant, or a slightly different copy, of a gene. You get one allele for each of your genes from your Mother, and one allele from your Father. If you know the genotype of both parents, you can predict genotype likelihoods of their offspring (allowing nutritional planning before and during pregnancy – how’s that for intelligent early intervention). I am heterozygous for MTRR A66G. A (adenine) has been replaced by G (guanidine) at the 66th position in 50% of my genes form MTRR. Thus 50% of my MTRR enzymes will be defective. I may have received the A66G allele from my Mother or from my Father. I am going to have trouble converting B12 in to methyl-B12, and this will compromise my health, but as 50% of my MTRR enzymes will function normally, my relative need for methyl-B12 is less than my relative need for methyl-folate, as 100% of my MTHFR enzymes are functioning abnormally. There are also Methyl Cycle Defects involving deletions or insertion of nucleotides (components of the genetic code) within a gene, and they are referred to by number. I am (+/+) for ACE Del16. This means that nucleotides that should be present at position16 of the ACE gene are not present. This heightens my risk for CV disease. Other Methyl Cycle Defects are named after the scientist who first described them, such as in VDR Taq or VDR Fok.
Punnett Square analysis allows us to predict the genotype of our offspring as a function of the genotype of both parents. Several examples are presented below. I’ve used myself as an example, so you’ve seen that I share with you several genetic liabilities – and I am not sick. Just because you have genetic predispositions it doesn’t follow that you have to be sick. I haven’t missed a day of work in 15 years and once a year I run a 26 mile Marathon – but I do try to take care of myself, I do take a lot of nutritional supplements, and I have applied the principles of heavy metal and hydrocarbon detoxification to myself. Now that I understand my Methyl Cycle predispositions, I will be in a better position to promote my own good health. We want to help you to do the same thing. Of interest, based upon my current understanding of the link between the Methyl Cycle and disease susceptibility, and what we are seeing in the Methyl Cycle findings of our own patients, I think that if I was born today I would likely suffer from Autism. But in 1955 there was little if any toxicity in the environment. The fish did not contain mercury, my Mom did not have Mercury amalgam fillings, and we were not then using Mercury containing vaccines, so my brain was allowed to develop normally. I will still be susceptible to Mercury and other toxins, but it is a lot easier to defend a fully developed and otherwise healthy physiology from Mercury, microbes, and other toxins, than it is to defend an immature or developing physiology from the same noxious influences.
|
Both Parents (+/+) |
Mother (+/+) |
Both Parents (-/-) |
Mother (-/-) |
||||
|
+ |
+ |
- |
- |
||||
|
Father (+/+) |
+ |
+/+ |
+/+ |
Father (-/-) |
- |
-/- |
-/- |
|
+ |
+/+ |
+/+ |
- |
-/- |
-/- |
||
|
When both parents are homozygous (+/+) all of their kids will be homozygous (+/+) |
When both parents are homozygous (-/-) all of their kids will be homozygous (-/-) |
||||||
|
|
|
|
|
|
|
|
|
|
Both Parents (+/-) |
Mother (+/-) |
Parents |
Mother (+/-) |
||||
|
+ |
- |
+ |
- |
||||
|
Father (+/-) |
+ |
+/+ |
+/- |
Father (+/+) |
+ |
+/+ |
+/- |
|
- |
+/- |
-/- |
+ |
+/+ |
+/- |
||
|
When both parents are heterozygous, |
With (+/+) and (+/-) parents, |
||||||
Cost issues - this will not be insignificant, nor can we expect much help from your health insurance. American Medicine focuses on doing procedures or prescribing drugs to deal with advanced pathology. This is what we get paid to do, so this is the medicine you get. The concept of using nutritional supplements and dietary change, specific to your genotype, to prevent or stabilize disease states such that you will require less drug therapy and invasive treatment, will not be well received or encouraged. Your insurer will consider such concepts to be “experimental” or not “evidence based”. There is no point in arguing with these people. The don’t get it. Treatment cost (basically the cost of your supplements) will be your responsibility. Early on this may run up to $200 per month, but as your sulfate and ammonia burdens fall, so will your requirement for supplementation. If your genetic challenge lies within the trans-sulfuration pathway (90% or you) our most important approach will be dietary change, and these foodstuffs are less expensive than the foods that you have been eating that have been making you sick. Also, please put all this in proper perspective. What did you pay for your car? Isn’t your health worth a fraction of what you paid for your car? What is a year of your life worth, to you and to your family? Do you wish to be vital and/or vocationally active in your 70s, or confined to a nursing home due to a health problem related to a Methyl Cycle predisposition? Now, if you are on board with me intellectually but are limited with respect to funds, we can try to stream line your program, and again, the harder you work on diet the less you will need to spend on supplements, but please do your best to follow the supplement program.
Lab testing will be important, and to some extent will be covered by your insurer. Vitamin D, homocysteine, and blood ammonia levels will likely change in response to our treatments and we will wish to follow these parameters; the cost of these blood levels will likely be covered. Urine sulfate and/or sulfite testing is critical; here you purchase the urine dipsticks and test yourself and record the results. We will need to follow your mineral status, as specific nutrients will be drawn in to pathways that were previously closed (we often see deficiencies in Molybdenum, Boron, and Copper). The best approach is a 24 hour urine study for nutritional minerals (with a concomitant measurement of toxic metals, which should start coming out on their own as your detox pathways open up). If a 24 hour urine is not possible we could use a first AM void “spot urine” or a red blood cell mineral assessment (go to doctorsdata.com for more information on these tests). Dr. Cowden has reconfigured the Asyra software to help us screen for Methyl Cycle abnormalities. If ammonia shows up, and you do not work with fertilizer or cleaning solutions, you likely have a problem in trans-sulfuration (CBS and or BHMT) or within the ammonia detoxification pathway (here the NOS enzyme). If sulfate and/or sulfite show up, then the problem likely lies in CBS/BHMT, while if we see sulfite but no sulfate, then SUOX (converts sulfite to sulfate) is likely the culprit. Asyra can never be as accurate as actual genomic testing, and at this point we have seen false positive and false negative Asyra Methyl cycle findings, but Asyra is low in cost and easy to carry out and lab testing is often high in cost and logistically difficult to carry out, so we will attempt to get the most information that we can out of the Asyra methodology. Regarding the urine sulfate determination, to our knowledge a high level of urine sulfate, especially coupled with a low blood homocysteine level, is indicative of a trans-sulfuration (CBS and/or BHMT) defect, but there could be conditions associated with a “false positive” urine sulfate. Also, if an “upstream” defect limits generation of homocysteine (AHCY +/+ or +/- does this), or if for any other reason you have been limiting animal protein in your diet, you could harbor a CBS defect and have a low urine sulfate (we do see this). Thus none of these screening tests can be perfect. We will need to interpret your test results in the context of what we know of your health and your genotype. Incidentally, you do not need to repeat your Methyl Cycle Genomics test – these findings will never change.
Individualized medicine, based upon analysis of one’s unique genetic code, is the future of medicine. We will do our best to provide you with this approach in 2008. Right now, our understanding of the Methyl Cycle allows us to translate your unique genomic pattern in to beneficial clinical recommendations. Over time, more science will become available, as will our expertise in treating abnormalities in your genotype. Your feedback can only make us better.
The brain behind Methyl Cycle is Amy Yasko PhD. Dr. Yasko’s area of clinical
expertise is in the treatment of Autism. You can learn much more form her
website holistichealth.com. We use Dr. Yasko’s lab for Methyl Cycle testing,
and many of the supplements discussed below can be obtained from her
holisticheal.com website. As Dr. Yasko points out, Methyl Cycle abnormalities
are not just the predisposing cause of Autism; they are the predisposing cause
of disease in general, the link between environmental toxicity and the
degenerative disease states that now plaque our society. Doctors like me are
attempting to utilize Dr. Yasko’s teachings in the care of individuals of all
ages (and to optimize their own health).
Now let’s discuss the individual genes, and our approach to the abnormal patterns that we see in our patients. 90% of the patients who we have tested returned with abnormalities in the trans-sulfuration pathway, specifically in the CBS gene, so we will start with the CBS up regulation.
Methyl Cycle Presentation Power Point Slides
This presentation was given in
2/15, within Module 1D of the American Academy of Anti-Aging and Regenerative
Medicine physician training program (the FAARFM behind my name indicates that I
have completed the course; now I have the privilege of teaching within three of
the modules). To view the slides please click the
corresponding tabs. Some day I will construct a 3-4 DVD audio-visual
presentation (but this takes time and a production cost of $5,000; if any of you
want to help here, the money will be placed in escrow and used only to produce a Methyl Cycle DVD presentation).
Methyl Cycle Slides Part One
Methyl Cycle Slides Part Two
Methyl Cycle, Antioxidant, and Detoxification Genomic Analysis - Getting Started
The cost of genomic testing has decreased. Through 23and me (23andme.com), extensive and useful genomic testing can be carried out for $99. Previously, through Dr. Yasko’s organization, we could obtain Methyl Cycle genomic testing alone for $550. Dr. Yasko’s report includes extensive discussion and a set of generic recommendations. 23and me provides only raw data. Useful information can be derived from this data, but you need to do the electronic footwork.
Generic information regarding Methyl Cycle Genomic Analysis is available on our website, heartfixer.com, and we have constructed fact sheets on many of the key genomic variants. Upon request, an individualized analysis with specific recommendations can be prepared for you (see Methyl Cycle and Detox Genomic Analysis at heartfixer.com).
The first step is to obtain
your genomic data. We can provide you with a Yasko kit, or you can go to
www.23andme.com. For $99 they will send you a saliva collection kit. You send
in the sample and 4-6 weeks later they will contact you (via e-mail) that your
results are in.
Your next step is to download your results (file) into www.geneticgenie.org
(.org – not .com) and obtain the Methylation Analysis and Detox Profiles (click
the tabs and follow their directions). Print out the reports in color and
forward them to the office. Mailing is better than faxing (if you fax the
report, make sure that the scanning intensity is light to prevent burn out).
23andme will not help you
do this, nor will the let us (they need to safeguard your confidentiality).
Please do not forward the raw data to us as we can do nothing with it.
23and me will provide you with some statistical data regarding your risk for
specific disease states, but this information does not pertain to the work that
we will do.
Next go to mthfrsupport.com, download your file, and for $30, you can print out pages and pages of genomic data (more detailed instructions below). Some of these genes I understand well, others I am learning, and others will be of interest to us in the future as we learn more.
Last, you can download your file at Nutrahacker.com. For a small fee, Nutrahacker will provide you with statistical data and a brief explanation of the key genomic variants that you bear (more detailed instructions below).. I find their analysis to be helpful.
If you are my patient and I suggest you undergo genomic testing, then I will use this information as we jointly make decisions as to the best approaches to you health concerns. I may suggest metabolic testing to help us understand how your genomic makeup (your genotype) is expressing itself within your current physiology (your phenotype.).
Testing that helps us integrate your genomic data in to your overall care includes:
A. The GenovaLabs NutrEval (covered by Medicare; $170 co-pay with commercial insurance) provides a great deal of information as to your nutritional status and level of oxidative and inflammatory stress and gives us some information regarding your organic pollutant and heavy metal burden.
B. A Drs. Data 24 hour urine mineral assessment covers nutrition mineral adequacy.
C. I frequently will
request serum iodine, Vitamin D, and ammonia levels.
D. SAMe and SAH testing is quite valuable. The
Health Diagnostics and Research Institute (www.hdri-usa.com - $350) can give us
levels of SAMe, SAH, and folic acid derivatives. Alternately, Doctors Data
gives us a less extensive but still useful Methylation Panel for $155.
E. A Sanesco study (covered by Medicare; $90 co-pay with commercial insurance)
will give us salivary cortisol values and urine neurotransmitter (serotonin,
dopamine, etc.) values.
F. For individuals with CBS/BHMT abnormalities, periodic monitoring of urine
sulfate is appropriate. The QuantoFix sulfate strips are obtained via amazon.com.
I view disease as an interaction between genomic predisposition, toxin/infection exposure, nutritional status, and diet/lifestyle. Knowledge as to our genomic predispositions, our strengths and weaknesses, helps in determining the best approach to resolving health challenges and in optimizing health.
James C. Roberts MD, FACC, FAARFM 5/25/15
MTHFR Support Genomic Report
23and me informed you that your genomic results (your file) was available. You have already printed out the Methylation Analysis and Detox Profiles at geneticgenie.com. The next step is to obtain your full mthfrsupport.com report.
A. Access your 23and me
account, open it, and log into you profile. Leave it open and open another tab
on your browser.
B. Go to mthfrsupport.com and sign up as a member (please write down or record
elsewhere your password and user name).
C. Once you have created an
account, click of the Sterling App, and pay the $30 fee (they only accept Pay
Pal). Save your 23and me report on your personal computer as a zip file, then
upload this file to mthfrsupport.com for a report. Step-by-step instructions
are available under “About Us”, then “FAQ”, then “Reports”. The 16th
bullet point down is “How do I transfer my 23andme raw data to you”?,
D. In a few moments a report will be generated. Save it as a PDF and print out
two copies in color (one for you and one for your office chart).
E. Mail one color copy to
our office. Do not e-mail this information to the office. Printing out these
reports is expensive in terms of staff time and ink (if time is of the essence
we can do this, but we will also charge you $25).
F. This date will be utilized in our future discussions and decision making.
How to Use Nutrahacker (from their website)
Step 1: Upload Your Data to NutraHacker
Use one of the following two methods to get started using NutraHacker.
Method 1: Connect directly to the 23andMe site using NutraHacker
(a) Click on the “Connect with 23andMe” button on the homepage www.NutraHacker.com.
(b) Grant NutraHacker access to your 23andMe genotype data.
(c) Confirm your profile information by entering your first and last names. This information is not stored in any way in the database. Click the button to let NutraHacker start processing your data.
Method 2: Upload your raw text file (this allows Ancestry.com users to obtain their nutrition report also.)
(a) Go to hhtps://www.nutrahacker.com/upload_text_file.php
(b) Select the raw text file for upload, then submit your data.
Step 2: Complete the Questionnaire
Fill out each question, answer either “Yes”, “No” or “Unsure/Decline to State”. Be sure to correctly enter your email address as well to receive a copy of your free detox information.
After submitting your questionnaire answers, you are taken to the checkout page where you can upgrade your account and gain access to your complete products.
Step 3: Purchase Access to Your Complete Information
There are currently two products available for purchase, and a discount if both are purchased at once:
Complete Mutation Report and Supplement Tool: 37USD if purchased alone
Carrier Status and Drug Response Report: 23USD if purchased alone
Combo price (16% discount) for both products purchased at the same time: 50USD.
For any
questions, comments or concerns, please contact
info@nutrahacker.com
Please forward a colored copy of your NutraHacker report to the office.
Individualized Methyl Cycle, Antioxidant, and Detoxification Genomic Analysis
My website and information sheets contain generic information, which may or may not be appropriate for you. An individualized report can be prepared, with specific instructions regarding treatment and suggestions as to further testing. Your health history and lab evaluation to date will be integrated into my report, which will be extensive. Thus the more information that you provide me, the better. If you wish, we can follow up with a phone consultation and/or office visit.
To start this process
please:
A. Contact my office, indicate your interest, sign the consent form, and prepay
$1500.
B. Obtain your genomic data from 23and me, genetic genie, mthfrsupport, and
NutraHacker, and forward the color copies to the office.
C. Please forward to the office:
1. Your health history, symptoms, concerns, and health wishes; the more detail
and information you give me, the better (when we as practitioners sense a great
deal of effort on the part of the patient, we tend to reciprocate). Reports
from your other practitioners and their recommendations will be helpful.
2. A recent picture (and if you wish, a picture when you were feeling well).
This helps me. It is easier to write about you if I feel that I am looking at
you.
3. The name of your insurer. Insurance will not pay for my analysis but
different insurers do or do not cover different diagnostic studies, and we try
to tailor study selection to minimize your out-of-pocket expense.
4. Laboratory data – if you think I might use it, then please send it. This
could include:
a) Standard labs, including homocysteine and Vitamin D (if these have not been
checked then it makes sense to do so now and forward the results).
b) Nutritional testing.
c) Hormone, adrenal, and neurotransmitter levels.
d) Infectious disease testing.
My turn around time is variable. My personal practice keeps me busy, and
periodically I need to spend time preparing and delivering presentations. Your
patience will be appreciated. Good work takes time and really good work may
take a little longer.
James C. Roberts MD, FACC, FAARFM 1/18/18
CBS (Cystathionine Beta Synthase) Explanation and Generic Plan of Action
Gene by Gene Approach – CBS +/- or +/+ with/without BHMT +/- or +/+
CBS
(Cystathionine Beta-Synthase) is discussed on pages 48-53 of Dr. Yasko’s book,
Genetic Bypass. Additional information is available on our heartfixer.com
website. You are +/+ (all of your CBS enzymes are abnormal) or +/- (half of
your CBS enzymes are abnormal) for one of the two CBS gain-of-function up
regulations and you may also be +/+ or +/- for one of the BHMT reduced-function
down regulations (which act like CBS up regulations). Homocysteine (and its
Methyl Cycle precursors) is thus being “pulled and pushed” down the
trans-sulfuration pathway, in this process generating excessive sulfur break
down products (sulfite and sulfate, which stimulate the stress/cortisol “fight
or flight” response), glutamate (which leads to glutaminergic excitotoxicity),
hydrogen sulfide (which produces brain fog), and too much ammonia (which
depletes BH4, leading to insufficient dopamine and serotonin production).
 This
deficiency in BH4 predisposes eNOS (endothelial nitric oxide synthase) to
convert arginine in to free radicals (superoxide and peroxynitrite) as opposed
to nitric oxide (atheroprotective vasodilator), predisposing you to hypertension
and cardiovascular and inflammatory disease states. Those of you with reduced
function alleles for the antioxidant enzymes SOD (superoxide dismutase), CAT
(catalase), GPX (glutathione peroxidase), and PON1 (paraoxonase) may be
challenged dealing with this superoxide free radical burden.
This
deficiency in BH4 predisposes eNOS (endothelial nitric oxide synthase) to
convert arginine in to free radicals (superoxide and peroxynitrite) as opposed
to nitric oxide (atheroprotective vasodilator), predisposing you to hypertension
and cardiovascular and inflammatory disease states. Those of you with reduced
function alleles for the antioxidant enzymes SOD (superoxide dismutase), CAT
(catalase), GPX (glutathione peroxidase), and PON1 (paraoxonase) may be
challenged dealing with this superoxide free radical burden.
I realize that this sounds awful but these are all issues that we can deal with, now that we understand their origin and biological significance. Also, we need to realize that the vast majority of these genomic variants lead to enzyme activity that is only slightly greater or lesser than normal wild type (“wild type” is the term used to designate the most commonly encountered or “usual” genomic structure of a given enzyme or molecule).
During normal physiology, metabolic flow down the CBS pathway generates the important anti-oxidant and detoxifying molecules glutathione, taurine and cysteine (all involved in maintaining vascular health). In response to oxidative (free radicals outstripping our antioxidant reserves) or inflammatory (infection or “perceived infection” with visceral obesity, leaky gut, and organic pollutants) stress, CBS activity will up regulate, allowing us to generate the glutathione and cysteine we need to neutralize this oxidative attack. However, as we drain homocysteine down the CBS pathway to generate antioxidants, we concomitantly drain homocysteine away from remethylation via the MTR and BHMT pathways, compromising our ability to recycle homocysteine back in to SAMe, the universal methyl donor.
In the absence of oxidative and inflammatory stress, we tend to remethylated homocysteine back in to SAMe, supporting methylation, while in the presence of these metabolic stressors (which Mother Nature views as life threatening), we sacrifice SAMe (compromising all methyl transfer reactions, including maintenance DNA methylation). This is OK short term, but through this mechanism chronic oxidative and inflammatory stress leads to accelerated aging, vascular and neurodegenerative disease states, and malignancy. Irrespective of our Methyl Cycle genomic status, if we wish to maintain good health we need to identify and resolve SAMe depleting chronic oxidative and inflammatory stress conditions.
SAMe itself stimulates flow down the CBS pathway (if you have plenty of SAMe you do not need to worry about recycling it); this is why we advise you not to begin SAMe (or push with measures designed to up regulate SAMe production) until your CBS/BHMT alleles have come under metabolic control. Otherwise you will “spend” the SAMe “just once” and precipitate sulfite/ammonia/glutamate excess.
SAMe has been used to treat lead overload (and presumably will work against mercury), as SAMe stimulates CBS, which inevitably converts homocysteine into glutathione. Thus if you feel poorly with Methyl Cycle supplements, it may be due to a “detox reaction” (or it may be due to increased production of sulfite/sulfate, ammonia, and hydrogen sulfide as the homocysteine generated from SAMe expenditure is pulled down an overactive CBS pathway).
While sulfate and sulfhydryl (-SH) bearing molecules are important in detoxification, sulfate/sulfite/-SH excess seems to block cellular up take of the key detoxifiers glutathione and cysteine (this is Dr. Yasko’s position; I can’t back this up from my review of the scientific literature but her position seems to work in Autistic kids). Endogenous detoxification is thus blunted (nearly all kids with Autism Spectrum Disorders bear CBS up regulations – why they are compromised by environmental toxins and the kid next door is just fine). Conversely, after we decrease your sulfate/sulfite pool, your detox pathways will open up (and why, if we move too fast, you will experience detox phenomena). As an illustration of this point, hair mercury (1st baby haircut) is lower in autistic kids than in non-autistic kids. As they improve, hair mercury increases. The problem is not greater than typical mercury exposure but the inability to remove it (retention toxicity). Irrespective of the biochemistry, we wish to lower sulfite/sulfate/ammonia before taking measures to increase glutathione.
The excess ammonia generated must be detoxified, and to do so BH4 (tetrahydrobiopterin) must be “spent”. This is a problem in that we need BH4 to generate neurotransmitters (serotonin to maintain calm/prevent depression and dopamine to maintain motivation and drive). Without BH4, we cannot convert arginine in to nitric oxide; instead vascular toxic free radicals such as superoxide and peroxynitrite are created, leading to hypertension and cardiovascular disease.
Ammonia is metabolized within the urea cycle, an enzyme pathway that utilizes several amino acids (ornithine, aspartate, arginine, and indirectly alpha-ketoglutarate) to break down ammonia. Systemic ammonia detoxification takes place in the liver, and thus individuals with advanced liver disease experience hyperammoniaemia, with attendant neurological dysfunction (tremor, confusion, impaired coordination). We can thus borrow from the gastroenterology community in our approach to the relative ammonia excess present in our patients with CBS/BHMT/MTHFR alleles (also giving me a chance to consult with our daughter, who is a gastroenterology fellow).
Intestinal microbes generate ammonia. Gastroenterologists use antibiotic therapy (Rifaxamin, a poorly absorbed antibiotic that does not enter the circulation) to sterilize the gut, thus blunting ammonia production. While we may recommend antimicrobial therapy if bacterial overgrowth is demonstrated on a CDSA (Comprehensive Digestive Stool Analysis), our approach here will be to take a probiotic 2-3 times a day to promote a balanced intestinal flora (not a bad idea for all of us to deal with the effects of antibiotics found in grocery store meats).
Charcoal absorbs ammonia generated within the GI tract, and thus taking charcoal at bedtime seems to lower one’s ammonia burden. Charcoal can also cause constipation, a huge negative here, as moving your bowels 2-3 times a day is important in detoxification and ammonia neutralization. Thus we recommend charcoal three nights a week with magnesium citrate and/or Vitamin C as needed to promote normal GI tract motility (adjust doses to obtain a balance between ammonia neutralization and proper GI tract function – too much magnesium or vitamin C pulls water into the intestines, leading to loose stools and diarrhea). Gastroenterologists utilize the cathartic lactulose to accelerate GI tract motility, blocking ammonia absorption; we can achieve the same end nutritionally with vitamin C and magnesium.
Ornithine/Aspartate supplementation (LoLa), administered IV or orally, is safe and effective in reducing ammonia in patients with advanced liver disease, and we can utilize this low cost approach to deal with ammonia excess in Methyl Cycle patients, starting with 1000 mg (1/3rd teaspoon) three times a day, increasing to one teaspoon as needed. Aspartic acid has a glutamate-like stimulating effect, and if one experiences agitation/anxiety than aspartate can be dropped in favor of more ornithine. Ornithine monotherapy has been used to increase exercise capacity in healthy people, as ammonia production is a metabolic consequence of energy utilization. These and other amino acids are best absorbed on an empty stomach or with a carbohydrate; concomitant protein intake will blunt their absorption. While we think of arginine as a means of improving nitric oxide production and endothelial function, arginine may also help metabolize ammonia.
The CBS C677T and A360A genes code for enzyme function that is pathologically up regulated. They are “always on” above that called for by the presence of oxidative stress. Of the two, the C677T allele is the most important, producing enzyme activity that is 10 fold greater than normal (your ancestors needed antioxidant support more than they needed methylation support; thus these SNIPs which direct homocysteine towards glutathione and away from SAMe regeneration). You thus suffer from “too much of a good thing” (glutathione and cysteine), “way too much of several bad things” (ammonia, hydrogen sulfide, and glutamate)” and impaired methylation (due to impaired SAMe recycling).
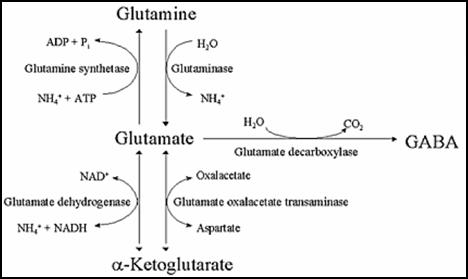
Dr. Yasko’s original teaching was
that CBS generated alpha-ketoglutarate (AKG) from homocysteine, and that
alpha-ketoglutarate could then be converted into glutamate, an excitotoxin. The
literature indicates that CBS generates alpha-ketobutyrate, not
alpha-ketoglutarate. However, nearly all patients with CBS up regulations
demonstrate high levels of glutamate, so Dr. Yasko may be on to something the
rest of us do not understand. In theory, alpha-ketoglutarate, in moderation, is
not a problem. We should be able to interconvert alpha-ketoglutarate into
glutamate, glutamine, and GABA (a calming neurotransmitter). However, when
alpha-ketoglutarate is in excess, or if toxic metals compromise the
interconversion enzyme (GAD1), then we suffer a buildup of the excitatory
neurotransmitter glutamate. Glutamate is involved in alertness and learning,
but excess glutamate leads to irritability and over-excitement; toxic levels may
play a role in seizure activity and cardiac arrhythmia (could this be why we are
seeing so much atrial fibrillation now then we were ten years ago)? Appendix
III (website) lists foods high in excitotoxic activity/glutamate/MSG.
CBS up regulations lead to an initial buildup of potentially neurotoxic sulfite, which is then metabolized by SUOX (Sulfite Oxidase) to the less neurotoxic (but still problematic at high levels) sulfate. SUOX activity requires molybdenum, which is thus depleted in CBS + individuals. Homogenized dairy products contain xanthine oxidase, which uses up molybdenum, and are best avoided or minimized. Vitamin E succinate, boron, and B12 are felt to stimulate SUOX activity.
As Methyl Cycle function (stated otherwise adequate SAMe and a high SAMe:SAH) is needed in the biosynthesis of Co-Enzyme Q10 and Carnitine, individuals + for CBS will likely be energy depleted, and here supplementation (in relation to your COMT/VDR status) with Co-Enzyme Q10, Carnitine, NAD+, or Ribose may be helpful.
BHMT (Zinc-dependent Betaine Homocysteine Methyl Transferase) directly methylates homocysteine back in to methionine, serving as a “back door” pathway to “pull” homocysteine away from the CBS “sulfate drain”. Thus if you bear CBS or BHMT abnormalities, it makes sense to support BHMT function. TMG (trimethylglycine) stimulate BHMT, and can be utilized if you are not overly sensitive to methyl group supplementation (based upon you COMT/VDR status).
Phosphatidylserine stimulates BHMT (and we also use it to moderate elevated cortisol levels), as does phosphatidylcholine (which we use to treat atherosclerosis, brain, and liver disease). 1/3rd of the SAMe generated through the Methyl Cycle is “spent” generating phosphatidylcholine (it takes three SAMes to generate one phosphatidylcholine). Phosphatidylcholine increases SAMe and the SAMe:SAH ratio by decreasing SAMe demand (the enzyme that spends SAMe and creates SAH to generate phosphatidylcholine is inhibited when phosphatidylcholine levels are high) and by increasing SAMe supply (by stimulating BHMT to remethylate homocysteine back in to SAMe), and it’s good for your blood vessels, brain, and liver. Phosphatidylcholine can be admixed with EDTA (which removes toxic metals from your body), creating a quite useful supplement. On the subject of “SAMe sparing”, another 1/3rd of our SAMe is spent generating creatine, a molecule involved in ATP energy recycling. Creatine supplementation is another means available to reduce SAMe and methyl group “demand” (please see Methyl Thieves section).
CBS in P-5-P (pyridoxal-5-phosphate, the active form of B6) dependent and utilizes serine as it converts homocysteine in to cystathione. Individuals with up regulated CBS activity are often deficient in serine and P-5-P, compromising other metabolic pathways (your NutrEval study will tell us if serine and/or P-5-P supplementation is in order).
Many of you with CBS and BHMT abnormalities will also bear MTHFR (compromising methyl-folate generation) and MTRR (compromising methyl-B12) abnormalities, and thus you will need and benefit from corresponding supplementation (with these molecules that you are having trouble making). However, if we treat you with methyl-folate, methyl-B12, or BH4, before we have the CBS problem under control (sulfite/sulfate levels low enough to allow for appropriate glutathione and cysteine assimilation) then we will be subjecting you to “incomplete detoxification”. You will feel great for 1-2 days, as beneficial neurotransmitters are generated. Detox pathways then open up, creating toxic intermediates that cannot be metabolized further due to the block in glutathione utilization (Dr. Yasko’s position) and possibly other genomic/nutritional blocks in Phase I and Phase II detoxification which we need to work on – and you will feel horrible. Thus we need to resist the temptation to treat your MTHFR/MTRR abnormalities until CBS/BHMT are under control. You’ve lived your entire life with a gene set that is maladaptive to the toxic environment of modern man. It will take us some time to change your internal environment to “bypass” these genomic challenges.
Plan of action for CBS +/- or +/+ (BHMT discussed further
in other sections)
(made out of context of your MTHFR, MTR, MTRR, COMT, VDR, and personal
health status)
To address this constellation of alleles I will recommend:
1. Moderate* animal protein intake (anything with eyes) and avoid sulfur rich
vegetables, sulfur containing supplements, and sulfur containing drugs (see
appendix II on the website and read Sulfites and Chronic Disease by Rick
Williams, available at the office or at
www.readingtarget.com/nosulfites).
2. Check the sulfate/sulfite content of your supplements and prescription agents
(many listed in the Williams book) and whenever possible switch to agents with
lower sulfate/sulfite content.
Gelatin capsules may contain sulfate; thus if possible switch to tablet or
powdered forms of key supplements.
3. Monitor urine sulfate levels (sulfate test strips can be obtained from Dr. Yasko’s holisticheal website; alternatively the QuantoFix strips are available at a lower cost on Amaxzon.com, and seem to work as well) every 3-7 days (or when you feel particularly good or poorly, or after adding a new treatment or changing your diet). Please chart the levels – this will be our primary measuring stick – our goal is a urine sulfate of 400 (one yellow and three pink) to 800 (two yellow and two pink). Low levels will allow an increase in methyl cycle supplementation and later the addition of BH4 and/or a liberalization of your diet. Conversely, persistent high sulfate spills indicates that your diet/treatment program needs further modification.
4. To neutralize ammonia (generated from animal protein), you can use Ammonia Support RNA* ½ dropper with meals and with methyl cycle supplements (relatively expensive), along with a charcoal supplement at bedtime every other evening, away from other supplements (charcoal may cause constipation, and here we can intervene with magnesium citrate and/or Vitamin C as needed to keep the GI tract moving - optimally twice a day - as charcoal may lead to constipation). Yucca, beginning at ½ capsule, twice a day, (or sprinkled on food containing protein), may help with ammonia detoxification. A probiotic twice a day makes sense to balance your gut flora. Ornithine/Aspartate 1000-3000 mg three times a day (taken away from other sources of protein) will stimulate the urea cycle, promoting ammonia degradation. If you experience irritability (aspartate is a stimulating amino acid) then switch to ornithine alone. Find the dose that makes you feel your best; there does not appear to be any toxicity associated with these amino acids (given orally or IV). While your ammonia level is likely not pathologically elevated, BH4 is used up in ammonia metabolism, so the less ammonia formed the better. Also, the better you are at breaking down ammonia, the more liberal we can be with respect to protein intake. We can measure serum ammonia and urine ammonia (within the NutrEval study).
*Dr. Yasko’s Ammonia Support product, to my understanding
(which may be incorrect), is an interference RNA, which blunts the production of
ammonia. I’m not exactly sure of the biochemistry here and as these products
are relatively expensive I do not emphasize the RNAs, but you can try them and
see if they help. You thus have the option of adding her CBS Support as well as
Ammonia Support RNA products to your program (in theory this would allow you to
take in more animal protein with less homocysteine “spillage” down the CBS
pathway).
5. Sparga Detox, 10 drops in water (wait at least one minute before consuming),
twice a day makes sense. Sparga was developed by fellow Cardiologist Dr. Lee
Cowden, specifically to address the CBS up regulations (see www.nutramedix.ec).
6. For nutritional support (pending the results of nutritional testing), a low-sulfate multi such as Dr. Yasko’s All in One, two twice a day, makes sense. To stimulate SUOX activity, please add Vitamin E Succinate 400 IU/day, sublingual hydroxy-B12 2000 mcg/day, and Molybdenum and Boron to your program. They may be taken individually as Molybdenum 500 mcg daily and Boron 3 mg daily, while Complete Mineral Complex (Designs for Health), 3 daily will cover the mineral base. Pyridoxal-5-phosphate (P-5-P, the active form of vitamin B-6) and the amino acid serine are the co-factors utilized by CBS as it degrades homocysteine down the trans-sulfuration pathway. At one point, we recommended avoiding P-5-P and serine in your program. However, P-5-P and serine are necessary for other metabolic and methyl cycle functions. Nutritional testing often demonstrates deficiency in both nutrients (especially in CBS + individuals), and most of you feel much better when P-5-P and serine are supplemented. Thus my position has changed. If you are not going to undergo nutritional testing, my recommendation is that you take P-5-P 34 mg (from 50 mg B6) and serine 500 mg twice a day.
7. Glutathione (and perhaps even more so its precursor cysteine) supplementation runs the risk off adding to your sulfite/sulfate burden. Right now this “good thing” could actually set you back. However, if we could convince your biochemistry to up regulate biosynthesis of glutathione, then your anti-oxidant and detox capacity will increase, with concomitant utilization of free sulfate/sulfhydryl groups – a double win for you. This can be achieved with the use of the Life Wave (needleless acupuncture) Glutathione patch. The Life Wave people have demonstrated an increase in Glutathione levels in relation to patch use (please see separate information sheet on Life Wave patch use). Toxicity testing** may also be carried out.
8. If you feel anxious or “wired up” (glutamate overload),
take GABA 500 mg or Zen (GABA 550 mg with Theanine 200 mg, a methyl donor) twice
a day. Individuals who need methyl groups (normal COMT and/or abnormal VDR Taq
alleles) will do better with Zen, while individuals who are methyl group
sensitive (COMT+) will likely do better with GABA. If they are helpful you can
double the dose. GABA does not work rapidly, but if you take it twice a day you
will build up a GABA reserve to balance the glutamate overload you are
experiencing due to your CBS up regulation. Magnesium supplementation may help
with GABA physiology and often helps with sleep.
9. If energy is low, or if deficiencies are identified on your NutrEval study,
we can supplement you with Co-Enzyme Q and Carnitine, keeping in mind that these
substances provide methyl groups, to which COMT + individuals may be sensitive.
Ribose 5 gm. 2-3 times a day and NADH 50 mg/day (or better yet NAD+ 100 mg/day)
do not provide methyl groups and should be well tolerated by all. A positive
response to ribose indicates that mitochondrial ATP energy production is subpar.
10. With respect to lab testing, we need baseline homocysteine and Vitamin D levels. After you have been on your program for 8-12 weeks, we can measure SAMe and SAH. The Health Diagnostics and Research Institute (www.hdri-usa.com - $350) can give us levels of SAMe, SAH, and folic acid derivatives (which will help us understand the affects of your FOLR, DHFR, SHMT, MTHFS, and MTHFD alleles). Alternately, Doctors Data gives us a less extensive but still useful Methylation Panel (which includes SAMe, SAH, homocysteine, and cysteine) for $155. Nutritional testing also makes sense. This could involve separate 24 hour urine studies for nutritional minerals and for ammonia/amino acids, or we might use the Genova Labs NutrEval. We need to make sure your mineral/nutritional stores are replete, and we are looking for low levels of ammonia, taurine, glutamate, and cysteine, to demonstrate that flow down the CBS pathway has been decreased to a physiologic level. Remember, we are not just analyzing genes. Rather we are evaluating genomic-nutritional-toxin interactions that affect the integrity of your methyl cycle and thus your overall health.
11. After sulfate levels have fallen (to a level that you
and I feel is optimal for you, based upon your clinical and genomic status),
then we will begin supplementation with methyl-folate, methyl-B12, and BH4.
This will take some time.
12. Be self-observant and keep records. Which foods, supplements, or other
maneuvers increase or decrease your sulfate spill? Which make you feel better
or worse? Always keep in mind that detoxification is not a fun experience. You
may need to accept some transient fatigue, malaise, and achiness to allow toxic
molecules to be cleared. Conversely, if detox symptoms are debilitating or
compromise your ability to work or care for your family, then we need to back
off on your treatments. Balance needs to be achieved. Rectifying your genomic
predispositions and detoxifying your system is not a sprint – it is a marathon.
And, as your genes are not going to change, and as the environment is not going
to become less toxic, you will need to be mindful of these principles for the
rest of your (long and healthy) life.
* How tightly should you restrict dietary protein? The
degree of protein restriction best suited for you will be in relation to your
personal health characteristics and your clinical and biochemical (urine sulfate
and ammonia levels) status. We need to keep in mind that Methyl Cycle Genomics
is not the sole determinant of your health. A low protein diet could become a
high carbohydrate, weight gain diet in an overweight individual with adult onset
diabetes, nor do we wish to create an essential amino acid deficiency (you need
amino acids for appropriate detoxification). Individuals with chronic,
unexplained illness or significant toxicity would do well to follow the “nothing
with eyes” diet until urine sulfate and ammonia levels have fallen; later on we
will liberalize your diet, while keeping an eye on these biochemical markers.
This maneuver isn’t fun and will require personal strength, but it also may turn
your health around. Individuals in whom the CBS up regulation is less important
(A360A as opposed to C677T, lower urine sulfate and ammonia levels, and better
overall health), could simply cut back on animal protein. In addition, the
greater representation of ammonia reducing (Yucca, Charcoal, LoLa, Ammonia
Support RNA) treatments in your program, the more protein you will be able to
take in without compromising your biochemistry. This is all about balancing
diet against treatment response and your other health concerns.
** The point of Methyl Cycle analysis/treatment is to help you become a more
efficient detoxifier. Toxicity testing (discussed in more detail in other
presentations and on heartfixer.com) thus makes sense. This could take the form
of:
A. The NutrEval provides us some information regarding organic pollutants and
gives us red cell (reflecting what your physiology has been exposed to over the
preceding three months) toxic metals ($170 with commercial insurance; fully
covered under non-HMO Medicare).
B. The US BioTek study gives us information on seven major organic pollutants
($126).
C. A formal provocative challenge ($250) gives us our best assessment of tissue
metal burden. Alternatively, an oral DMPS challenge ($125) could be carried out;
this study provides less extensive information but can be carried out at home.
D. The Hunt Digital picture approach ($350) assesses for toxicity (and other
health challenges) by analyzing the frequencies emitted by your body (and tells
us which Digital Homeopathic Patches would be most appropriate). I can’t prove
this approach with an allopathic lab test but it has been quite helpful in
solving complex medical problems in my personal patients. Dr. Hunts CD is
available for your review and you can go to www.auraexplorationpatches.com for
additional information.
E. While on the subject of energy medicine, learn about the benefits of static
magnetic field therapy (I sleep on a 20 gauss static field sleep pad - see MME
section on heartfixer.com or go to magneticosleep.com). The ground/earthing
approach is low in cost and likely has value for all of us. My colleague Dr.
Sinatra wrote a book on this subject (heartmdinstitute.com).
OUR FIRST GOALS WILL BE TO REDUCE YOUR BURDENS OF
SULFITE/SULFATE, AMMONIA AND GLUTAMATE
James C. Roberts MD FACC FAARFM 5/25/15
CBS: Cystathionine Beta
Synthase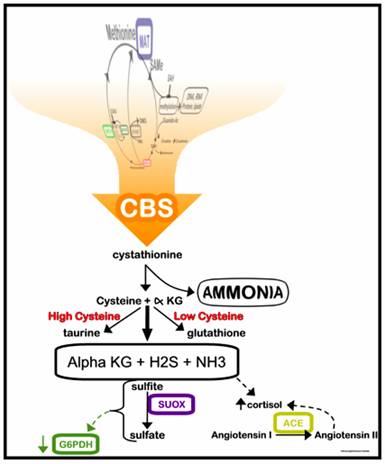 (Older Explanation)
(Older Explanation)
CBS initiates the trans-sulfuration pathway,
converting homocysteine in to cystathionine and its downstream metabolites.
This is the most important Methyl Cycle defect and is present in 90% of the
patients who we have tested. The CBS defect is an up regulation. CBS is
operating at up to ten times its normal rate. Homocysteine and all of the
upstream methyl cycle precursors will be “pulled down the CBS drain” to produce
toxic levels of cystathionine metabolites. The C699T and (to a somewhat lesser
extent) A360A defects are associated with CBS up regulation. Homozygotes (+/+)
will be more severely affected than will be individuals heterozygous (+/-) for a
CBS abnormality. We treat CBS ( +) individuals with dietary animal protein and
sulfate restriction and supplements designed to neutralize ammonia and speed up
clearance of sulfite/sulfate. Laboratory findings consist of an elevated urine
sulfate level, a low or low normal blood homocysteine level, an elevated or high
normal blood ammonia level, and positive findings of ammonia, sulfite, or
sulfite upon Asyra testing. My initial observation is that individuals with
high heavy metal burdens upon provocative challenge testing are likely to be CBS
positive. CBS (+) individuals will be intolerant to sulfur containing drugs,
nutritionals, and foodstuffs (I am +/- for CBS A360A and cannot tolerate DMPS or
glucosamine sulfate. A cold beer tastes great but I do not like wine, which is
high in sulfite).
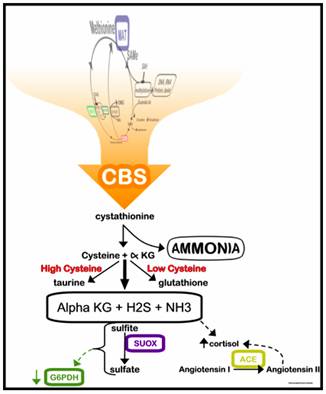
Biochemistry – The 10-fold up regulation in CBS generates sulfur breakdown products (sulfite and sulfate, which stimulate the stress/cortisol “fight or flight” response), excess ammonia (in the process wasting BH4 which is used up detoxifying ammonia), hydrogen sulfide (producing “brain fog”), and alpha-keto glutarate (leading to “excitotoxicity”). The G6PDH enzyme system may be affected, leading to abnormalities in sugar control. Methylation intermediates will “fall through this drain”, so the entire system suffers; our defenses against viral invasion and toxicity suffer. Co-Q10 and Carnitine generation will fall off due to impaired methylation, and ATP levels fall, robbing you of energy.
Ammonia is produced during the metabolism of dietary protein. The CBS up regulation drains methyl cycle intermediates in to ammonia, more ammonia than your system can handle. Ammonia detoxification is metabolically expense, using up two molecules of BH4 per molecule of ammonia. BH4 is necessary to generate neurotransmitters (dopamine, serotonin, and norepinephrine) and nitric oxide, our key vasoprotective molecule. Thus it is easy to see how a CBS up regulation, by generating ammonia and depleting BH4, can set you up for neurological, psychological, and cardiovascular disease states. We cannot change your DNA. We cannot stop CBS from generating excess ammonia, but if we restrict animal protein in your diet, we can decrease your ammonia burden, preserving BH4, such that you can start making neurotransmitters and nitric oxide again – in other words, we can compensate for your genetic challenge. The herb Yucca, Dr. Yasko’s Ammonia support RNA product, and supplementation with charcoal and carnitine will bind up or neutralize ammonia, and add to your dietary efforts.
Sulfite is neurotoxic. Sulfite will be over produced by the CBS up regulation, and then requires conversion in to the less toxic sulfate molecule by the enzyme Sulfite Oxidase (SUOX). SUOX can easily be overwhelmed. Molybdenum is required for SUOX function, and is typically depleted in CBS (+/+) or (+/-) individuals. Molybdenum supplementation (3 drops or 75 mcg of e-lyte Molybdenum twice a day), Boron 3 mg/day, Vitamin E succinate 400 IU/day, and hydroxy-B12 2000 mcg/day are also utilized to speed up SUOX activity.
While sulfate is less toxic than is sulfite, it will stimulate the adrenergic (fight or flight) limb of the autonomic nervous system and stimulate a cortisol stress response, revving you up into an unrelenting biochemical overdrive. If you have a CBS defect, we need to restrict your sulfur intake, at least until your urine sulfate (and your body sulfate burden) has decreased. The amino acids methionine, taurine, and cysteine all contain sulfur; they are concentrated in animal protein (thus the restriction on animal protein intake). Many nutritional supplements (MSM, N-acetyl cysteine, glutathione) that are good for most people are a problem for you. While certain aspects of your health will benefit from these agents, they will add to your sulfate/sulfite overload problem, adversely affecting the Methyl Cycle Defect that is the common denominator to all of your health problems. Many drugs are loaded with sulfur (sulfates, sulfites, metabolically active sulfur), so if you are CBS positive and I treat your hypertension with the diuretic hydrochlorothiazide, your diabetes with the sulfonylurea drug glipizide, and your urinary tract infection with a sulfa containing antibiotic, I will be lowering your blood pressure, lowering your blood sugar, and clearing bacteria from your bladder, but I will also be adding to your sulfate burden, compromising your biochemistry, and contributing to an ongoing decline in your health. I will be treating the manifestations of an underlying problem and at the same time adding to the underlying problem. If I treat your Mercury overload with DMSA or DMPS, I will remove a toxin from your body, but if you are CBS (+), I will be adding to your sulfate/sulfite pool, and sulfate/sulfite overload due to the CBS up regulation is likely playing a key role in your sensitivity to heavy metals and/or your inability to clear them. We can avoid this. We can hold sulfur containing agents until your sulfate burden has come under control. Learn all you can about the sulfur content of foodstuffs, supplements, and prescription drugs. Sulfites and Chronic Disease by Rick Williams (available at the office or at www.readingtarget.com/nosulfites) is an invaluable resource. Do not expect us to know the sulfur content of foodstuffs. Some tips on low sulfur eating are included at the end of this document, but do not expect us to tell you what to eat. We can’t do this. We do not have this knowledge. Please attend our monthly Methyl Cycle support groups meetings, and you may sign up for individual (or group) dietary change counseling. It is your responsibility to become expert in this area. I will work with you to phase out high-sulfur drugs and nutritionals from your program, but don’t expect me to get in right every time – please study your food, drug, and supplement labels.
Excitotoxicity – The CBS up regulation leads to excess production of alpha-ketoglutarate, which is converted in to glutamate, a stimulatory neurotransmitter. Under normal circumstances, glutamate will be converted in to GABA, a calming neurotransmitter, but the enzyme systems that convert glutamate in to GABA are compromised by lead and mercury, the clearance of which seems to be compromised in individuals with methyl cycle defects (here is a situation where dysfunction of a genetically abnormal enzyme leads to acquired dysfunction of a genetically normal enzyme system). The result is “excitotoxicity”, stimulatory behavior in autistic kids (“stims”) and anxiety and sleeplessness in adults. We approach this problem by limiting alpha-ketoglutarate and glutamate rich foods from your diet (more on Excitotoxicity to follow; diet tips in appendix) and by supplementing you with GABA, aiming to restore GABA:Glutamate balance. GABA is initiated at 500 mg once or twice a day, advancing the dose as you see fit by your response.
Abnormalities in BHMT (Betaine-Homocysteine Methyltransferase) aggravate and frequently co-exist with CBS defects. BHMT mediates the “backdoor” pathway of homocysteine metabolism, drawing homocysteine away from the trans-sulfuration pathway that is up regulated in CBS (+) individuals. A defect in BHMT, will thus mimic or add to a CBS defect. BHMT can be stimulated with Phosphatidylserine, Phosphatidylcholine (which is combined with the metal chelator EDTA in Lipophos EDTA), and the methyl donor TMG (Trimethylglycine), and one or more of these agents will be included in our treatment program for CBS (+) and/or BHMT (+) individuals.

In a
sense, the key ultimate consequence of CBS/BHMT abnormalities will be BH4
deficiency. By neutralizing the consequence of your CBS up regulation and/or
BHMT down regulations, your BH4 status should begin to return towards normal.
We also can supplement you with BH4. It is strongly recommended that BH4
supplementation be held until all other Methyl Cycle pathways have been
optimized. Pharmacological doses (200 mg/day) of BH4 has been shown to be safe
and effective when used to treat endothelial dysfunction in hyperlipidemic
individuals, and in dealing with Methyl Cycle defects, far lower nutritional
doses (2.5 mg four times a day) are typically employed, but here a little bit of
BH4 can go a long way, and we need to be prepared. If long-closed detox
pathways are suddenly opened up, you could experience a detox reaction, so we
need to get the rest of your systems up and running before we open these closed
gates. If neurotransmitter generation suddenly comes back on line, and you are
taking an anti-depressant drug or nutritional that preserves neurotransmitter
levels, you could experience a neurotransmitter surge if we have not cut back on
the drug dose. If we give you BH4 before you are ready, you will feel great for
a day or two, and then “crash”, with fatigue and malaise, as we attempt to spin
other metabolic wheels forward that are still stuck in the “off position”. Thus
we need to be patient, take things step by step, with the long goal in mind.
Energy
Production
will falter. To generate ATP energy, you need Co-enzyme Q10 and Carnitine, but
to manufacture these co-factors you need methyl groups, which tend to be in
short supply in individuals with Methyl Cycle defects. To make matters worse,
when energy is in short supply, homocysteine is shunted in to ammonia, hydrogen
sulfide, and alpha-ketoglutarate, and not in to its one beneficial metabolic
product, glutathione. NADH, Carnitine, Co-enzyme Q10, and its non-oxidizeable 1st
cousin Idebenone will all help with ATP energy production, and their use makes
sense in patients with CBS up regulations, especially if they have
cardiovascular disease. (I am getting ahead of myself, so skip this entry if
you wish, but the latter three agents also can serve as methyl donors. We will
be more liberal with their use in individuals who are COMT (-/-), who need
methyl donors, and more conservative in their dose in individuals who are COMT
(+/+), who will be more sensitive to methyl group supplementation). Ribose
increases ATP regeneration in individuals with cardiovascular disease or other
conditions associated with energy deficiency, and can be taken as well.
SUOX (Sulfite Oxidase) converts sulfite in to sulfate. I am (+/-) for
SUOX and (+/-) for CBS, meaning that I am overproducing sulfite and having
trouble converting sulfite in to less toxic sulfate. I will thus need to be
particularly vigilant with respect to supporting SUOX function. Molybdenum, in
short supply in CBS + individuals, is also used up by the enzyme xanthine
oxidase, a free radical generating enzyme system that plays a role in gout (it
produces uric acid which precipitates in your joints to cause the pain and
inflammation of gout). Xanthine oxidase is present in pasteurized milk, which is
best avoided or minimized in CBS (+) individuals. A note regarding
nomenclature; a defect in a Methyl Cycle enzyme is typically described with a
(+). I am homozygous (+/+) for MTHFR C677T so 100% of my MTHFR enzymes are
defective. For reasons that make no sense to me, someone decided that the
normal designation for the SUOX gene should be (+/+); thus if you are (-/-) for
SUOX you are homozygous abnormal. This is the only gene where (-/-) is abnormal
and (+/+) is normal. In my shorthand, I will refer to any defect in any Methyl
Cycle gene as a (+). If I refer to an individual as CBS (+), I am referring to
an individual with a CBS abnormality, either (+/+) or (+/-). To keep things as
clear as possible (and believe me I am trying) I will also can refer to
individuals who are abnormal for SUOX as SUOX (+).
My general treatment program for CBS (+) individuals and
for BMHT (+) individuals who are overproducing ammonia and sulfite/sulfite will
consist of:
1. Restrict animal protein (anything with eyes) from your diet and limit your
exposure to sulfur group containing drugs and nutritionals.
2. To squelch ammonia, supplement with Yucca, ½ capsule twice a day (sprinkled
on food containing protein), Ammonia Support RNA ½ dropper with meals, and a charcoal supplement at bedtime (away from other
supplements; magnesium citrate may be used as needed to keep the GI tract moving
as charcoal may lead to constipation).
3. Switch to a multi that does not contain B6 (B6 stimulate CBS; the P-5-P form
of B6 is less of a problem – Dr. Yasko’s NHF multi is low in B6 - take two
tablets three times a day). Additional mineral support will be needed and
here we start with Trace Minerals Complex
at 4 drops/day.
4.
To stimulate SUOX begin Molybdenum 3 drops twice a day, Boron 3 mg/day, Vitamin
E succinate 400 IU/day (contained in the NHF multi), and hydroxy-B12 2000
mcg/day.
5. Supplement with GABA 500 mg once or twice a day to blunt excitotoxicity; if
you feel that GABA is helping you can increase the dose.
6. To
increase energy production (this step is less critical and can be omitted for
cost containment, especially in individuals not troubled with CV disease)
supplement with NADH 5 mg, Co-Enzyme Q10 100 mg or Idebenone 100 mg, Carnitine
500-1000 mg daily, and Ribose 5 grams in water, two to three times a day.
Co-Enzyme Q10, Carnitine, and Idebenone all provide Methyl groups, and are thus
of additional value to COMT (-) and/or VDR Taq (+) individuals.
7. Additional measures designed to speed up the “back door” BHMT reaction will
be discussed later.
8.
Check and record your urine sulfate level every 7 days. Our goal is to reduce
your reading to 400 mg/L (one yellow and three pink squares) or at least to 800
mg/L (two yellow and one pink), and then to keep it there for two months (at
which time you will feel better). Measures that
decrease your sulfate burden are beneficial. Conversely, any measure that
increases your sulfate burden is either inappropriate or is being added to your
program prematurely. A persistent reduction in your urine sulfate level will
open the door to SAMe and/or BH4 supplementation and an eventual liberalization in your
diet. Your urine sulfate score will thus be our primary measuring stick.
9. If not done already, we need to check your baseline blood homocysteine,
ammonia, and Vitamin D levels, along with kidney and liver chemistries (if not
done recently).
10. Consider wearing the Life Wave Glutathione patch 4-6 hours each day,
removing the patch if you feel poorly (this would reflect a detoxification
reaction - see our info sheet and lifewave.com/chc), the idea here being to use
up free sulfur groups to generate Glutathione.
11. In 8-10 weeks we will likely wish to:
a. Repeat some of the lab work.
b. Carry out 24 hour urine studies for ammonia and amino acids, with a second
study for toxic and nutritional minerals, and possible a SpectraCell
intracellular nutritional assessment. We will use the results to modify our
nutritional measures, specifically looking for nutrients that have been drawn in
to your now open pathways, nutritionals that will now require more intensive
supplementation. Favorable results will also allow us to back off on the dose
of now less necessary supplements.
Gene by Gene Approach and Plan of Action – MTHFR C677T +/+ or +/-
(Generic, Non-Individualized
Recommendations - Individualized Recommendations can be prepared upon
request)
Here ½ (+/-) or all (+/+) of your MTHFR enzymes are having trouble converting folic acid (or more precisely 5,10-methylene tetrahydrofolate) into 5-methyl folate. Without 5-methyl-folate (which we will shorten to methyl-folate) MTR cannot methylate homocysteine in to methionine and SAMe regeneration will be compromised. Methyl folate has another role - it can neutralize peroxynitrite. When NOS (nitric oxide synthase) is not functioning normally (i.e. when BH4 is deficient or if eNOS reduced function alleles are present), arginine is converted not in to the vasoprotective molecule nitric oxide, but rather in to the damaging free radicals superoxide and peroxynitrite. Superoxide (neutralized by Vitamin C) can further degrade nitric oxide, while peroxynitrite degrades BH4 (stimulating a vicious cycle). Methyl folate can neutralize peroxynitrite, thus sparing BH4, keeping it available such that NOS can generate nitric oxide, the vasoprotective molecule that we need - thus the need to maintain healthy production/levels of methyl folate. In addition, supplemental methyl-folate can be metabolized by MTR (Methionine Synthase, which tacks on to homocysteine a methyl group obtained from methyl-folate) to THF (tetrahydrofolate), and then “back converted” by DHFR (Dihydrofolate Reductase) to DHF (dihydrofolate), in this process “recharging” spent BH2 back into useful BH4. Methyl-folate can also “stand in” for BH4 when the later is in short supply. Methyl-folate is thus an extremely important biomolecule. We can easily bypass the MTHFR C677T block with 5-methyl folate supplementation. Sources of 5-methyl folate include Folapro (800 mcg 5-methyl folate), Metanx (5-methyl folate 2.8 mg, P5P 25 mg, and methyl-B12 2 mg), Deplin (7.5 mg 5-methyl folate), and Cerafolin NAC (5-methyl folate 5.6 mg, NAC 500 mg, and methyl-B12 2 mg). Riboflavin deficiency may be a key issue in individuals with C677T alleles, as this SNIP codes for a MTHFR enzyme that does not bind well to its FAD (riboflavin based) co-factor. Individuals +/+ for MTHFR C677T with above average riboflavin nutriture typically have normal homocysteine levels, while individuals low in riboflavin and + for C677T will have the highest homocysteine values. We can assess for riboflavin and folate sufficiency with NutrEval testing. We can assess for riboflavin and folate sufficiency with NutrEval testing. Serum homocysteine gives us information regarding methyl-folate sufficiency (keeping in mind that individuals with CBS up regulations may have low homocysteine levels even in the presence of methyl-folate and/or methyl-B12 insufficiency).
Plan of Action – MTHFR C677T +/+ or +/-
(made out of context of your CBS, BHMT, MTR, MTRR, and personal health status)
1. Supplement with methyl-folate, at a dose commensurate with your genomic and homocysteine status (400-800 mcg/day if you are +/- and 800-1600 mg/day if you are +/+, of if homocysteine is markedly elevated).
CBS + and/or BHMT + warning – If you harbor these genes, you may be compromised by a sulfate/ammonia/glutamate burden. If we supplement you with methyl-folate (or methyl-B12) before these issues are addressed you will feel great for 1-2 days (honeymoon period) and then you will begin to experience adverse symptoms on the basis of incomplete/disordered detoxification and/or increased generation of sulfite/sulfate/hydrogen sulfide/ammonia.
2. Riboflavin 50-100 mg/day, ideally with follow-up testing of folate and riboflavin status with a NutrEval study.
3. Another idea – Far Infrared Sauna promotes detoxification and increases BH4 levels.
Gene by Gene Approach and Plan of Action – MTHFR A1298C +/+ or +/-
Dr. Yasko describes MTHFR A1298C as an abnormality in the SAMe binding site of MTHFR that compromises the “backward reaction” that generates BH4, a problem in that BH4 is used up detoxifying ammonia (which you are making in excess if you bear a CBS up regulation). This “backward reaction” is not supported by other authors, but a pathway does exist (mediated by DHFR) such that poor methyl-folate status will compromise BH4 recycling. Methyl folate supplementation may stimulate the backward reaction and will help regenerate BH4, and methyl-folate can “stand in” for BH4 when the latter is depleted. After your urine sulfate levels have fallen we may advance methyl-folate or add in BH4 supplementation. Efforts to lower ammonia production and/or increase ammonia metabolism make sense here (see CBS up regulation section). Far Infrared Sauna increases BH4 production and promotes detoxification and could be utilized here. MTHFR A1298C may also be associated with a weak impairment in methyl-folate generation, which we can bypass with methyl-folate supplementation.
James C. Roberts MD, FACC, FAARFM
3/5/16
MTHFR C677T: 5,10-Methylenetetrahydrofolate Reductase (Þ 5-Methyl-Folate)
The MTHFR C677T defect is easy to understand and even easier to treat, but the consequence of the MTHFR abnormality in kids appears to be profound, such that the parents of Autistic kids add a few more vowels to MTHFR in naming it. Folate absorption and processing is discussed below, but as a general rule dietary folic acid is not in short supply and is readily converted into its active form, tetrahydrofolate (THF). SHMT (discussed below) converts THF in to 5,10-methylene tetrahydrofolate, which is acted upon by MTHFR to generate 5-methyl-folate. Methyl-folate is then utilized by MTR (Methionine Synthase) to remethylated homocysteine back in to Methionine for SAMe regeneration. When MTHFR is dysfunctional, homocysteine cannot be remethylated, SAMe falls, the SAMe:SAH ratio falls, and then the Methyl Cycle fails, leading to birth defects and autism in kids and atherosclerosis, malignancy, and neurodegenerative conditions in adults. MTHFR C677T is often the rate limiting step.
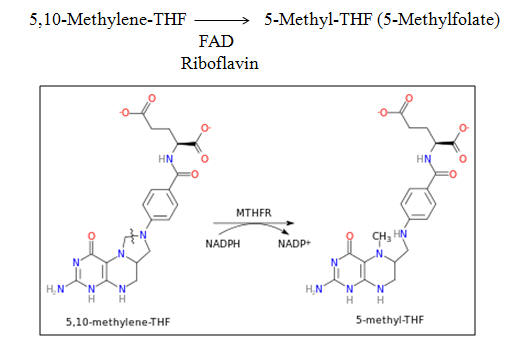
The MTHFR C677T polymorphism refers to the substitution on thymine for cytosine at the 677th base pair position within the transcribed region of the MTHFR gene. The corresponding MTHFR enzyme bears the amino acid valine, as opposed to the usual or "wild type" alanine at the 222nd amino acid position within the enzyme.
Individuals who are (+/+)
for MTHFR C677T (10% of the population, including me) have a great deal of
trouble using dietary folic acid to detoxify homocysteine, as we cannot
efficiently convert dietary folic acid into its 5-methyl folate form. Elevated
homocysteine leads to free radical stress, vascular plaque formation, abnormal
clotting, and an increased risk for cardiovascular and neurological disease –
yikes! If you are (+/+) or (+/-) for MTHFR (another 20% of the population),
supplementation with folic acid is not the best answer. Higher doses of
supplemental folate (or a diet rich in folate-providing fruits and vegetables -
more on this below) would be required to "push" enough 5,10-methylene
tetrahydrofolate through the sluggish MTHFR TT pathway. However,
low dose 5-methyl folate supplementation will bypass this defect with 100%
efficacy. If you have a MTHFR C677T defect, we can overcome it with
5-methyl folate supplementation.
As you can see from the
chart to the left, MTHFR requires a riboflavin-based co-factor FAD (FAD is
involved in numerous physiologic functions). Riboflavin is used up as
MTHFR converts 5,10-methylene tetrahydrofolate
in to methyl-folate. Stated otherwise, high dose folic acid
supplementation can lead to riboflavin deficiency (compromising other aspects of
your biochemistry). This may explain why studies using high dose folic
acid to lower homocysteine did lower homocysteine but did not always improve
clinical outcome - the high dose folic acid created riboflavin deficiency. Conversely optimal riboflavin nutriture will
ameliorate (and possibly resolve) any impairment in methyl-folate generation due
to MTHFR C677T + status.
The charts bellow pertain to an epidemiologic study carried out in healthy young people in Ireland. 12% of the subjects were +/+ for MTHFR C677T (referred to in the charts as TT), 45% were +/- (referred to as CT), and 43% were -/-, or normal MTHFR function "wild type" (referred to as CC). As you would expect, homocysteine levels were greater in CT and TT subjects vs. those with wild type, CC status. 28% of these healthy young people were deficient in riboflavin. The researchers stratified riboflavin nutriture into terciles (lower, middle, and upper third), and correlated riboflavin status with MTHFR status as determinants of homocysteine. You can see that MTHFR TT and CT status increased homocysteine when riboflavin status was sub par. Conversely optimal riboflavin intake was associated with normal homocysteine, irrespective of MTHFR genomic status. Thus the key problem with C677T is an increased need for riboflavin. When our diet was rich in fruits and vegetables we all got in enough folic acid and riboflavin and MTHFR status was not a health issue. When we decided to favor processed foods, sugar, and trans-fats we began to experience suboptimal folate and riboflavin deficiency and MTHFR TT individuals got hurt first, often not making it through gestation! We put a man on the moon but aren't smart enough to eat correctly, so we die during gestation.
Now, Mother Nature never does anything without a purpose, and as a MTHFR TTer, I am pleased to announce that the frequency of my genotype is increasing in the population. That's right, more and more of us (in Western societies) are now TT. The charts below describe the distribution of CC, CT, and TT status over time in a stable population group is Spain. .
 9-15% of the
subjects in the 21-40 year old range were TT while 27-30% of the younger
subjects carried the TT genotype; 16-20 year olds were in between. What is
the explanation?. As we will discuss below, MTHFR TT status is not really a bad
thing if you are living life and eating food as Mother Nature planned for us.
Problems, big problems, occur if you do not listen to Mother Nature, or
pertaining to the prevalence of TT status in this Western population, if you are TT and your Mother did not!
9-15% of the
subjects in the 21-40 year old range were TT while 27-30% of the younger
subjects carried the TT genotype; 16-20 year olds were in between. What is
the explanation?. As we will discuss below, MTHFR TT status is not really a bad
thing if you are living life and eating food as Mother Nature planned for us.
Problems, big problems, occur if you do not listen to Mother Nature, or
pertaining to the prevalence of TT status in this Western population, if you are TT and your Mother did not!
If you are TT and your Mother's diet was low in folate and/or riboflavin, you are at increased risk for a terminal birth defect, and you may not survive gestation. Conversely, if your Mother's nutritional status was adequate you will develop normally. Western women (and men, but we are not important in this analysis) stopped listening to Mother Nature in the mid-1900s. We switched form a plant based, real food diet to low nutriture processed foods, and we as a society became B vitamin deficient, and TT individuals were lost during gestation. Twenty years ago we realized our mistake. The link between maternal B vitamin insufficiency and neural tube defects was accepted (this was obvious decades earlier but Medicine scorns nutritional supplementation), and B vitamin supplementation during pregnancy became the norm. TTers are now more likely to make it through gestation, and now our representation within the gene pool has been restored.
Now, why would Mother Nature want us TTers in the first place? What good is there in not being an efficient methyl-folate generator? Well, being MTHFR TT dramatically decreases your risk of several malignancies. Mother Nature always has a good reason for everything she does. We just need to figure it out. Now is a good time to revisit the functions or goals of the Methyl Cycle.
The function of the Methyl Cycle is to maintain (current health status)
appropriate levels of:
A. SAMe, along with a high SAMe:SAH ratio, necessary for biological methylation.
B. BH4, need to generate neurotransmitters and nitric oxide.
C. The antioxidant/detoxification molecules cysteine, taurine, sulfate, and
glutathione.
D. Purine and Pyrimidine bases for DNA and RNA generation.
We take in
folic acid and convert it to methyl-folate, not to lower homocysteine but to
generate SAMe, antioxidant molecules, BH4, and the purine and pyrimidine bases
needed to make DNA. All of these goals must be met. If we generate plenty
of glutathione to deal with oxidative stress but don't make DNA correctly then
we risk malignancy. Balance must be achieved. MTHFR converts 5,10-methylene tetrahydrofolate
in to methyl-folate. Take a look at the chart to the left and focus on 5,10-methylene tetrahydrofolate
(Methylene THF on the chart). Please note that this "raw material" folate can be
converted into thymidine, to generate pyrimidine DNA bases (by thymidinylate
synthase) and by MTHFD in to purine DNA bases.
Consider what might happen if folate was in short supply and if MTHFR was overly rapid converting Methylene THF into methyl-folate. MTHFR is activated by SAMe deficiency. This might occur if CBS is chronically up regulated (when CBS is up regulated, homocysteine is drawn away from remethylation to reconstitute the SAMe pool). CBS C699T and A360A variants code for persistently up regulated CBS activity. Oxidative and inflammatory stress up regulate CBS activity (you need the glutathione to survive this imminent threat to your survival). In these situations, all of your Methylene THF will be converted in to methyl-folate and little will be left for DNA generation, placing you at risk for malignancy (and chronic inflammation and oxidative stress do lead to malignancy). Mother Nature designed MTHFR T to put a brake on this process, to protect us from impaired DNA formation. This is a good thing!
 The graphic to your left pertains to a
study of MTHFR genotype in US Health
Professionals with colorectal cancer (blue) vs. age-matched controls (red)
without cancer. Your can see that a greater percentage of cancer free
control subjects were MTHFR TT. TT is protective. The graphic to
your right looks at relative risk for colorectal cancer. Simply being TT
decreases risk by » 40%.
High alcohol intake (alcohol compromises Methyl Cycle function) increases risk,
while high methionine (spares folate as methionine is a building block for SAMe)
decreases risk. This all makes sense.
The graphic to your left pertains to a
study of MTHFR genotype in US Health
Professionals with colorectal cancer (blue) vs. age-matched controls (red)
without cancer. Your can see that a greater percentage of cancer free
control subjects were MTHFR TT. TT is protective. The graphic to
your right looks at relative risk for colorectal cancer. Simply being TT
decreases risk by » 40%.
High alcohol intake (alcohol compromises Methyl Cycle function) increases risk,
while high methionine (spares folate as methionine is a building block for SAMe)
decreases risk. This all makes sense.
 This
set of graphics takes our analysis a step further. Alcohol blocks several Methyl
Cycle enzymes (especially MTR which utilizes methyl-folate to remethylate
homocysteine back in to methionine). TT individuals with low alcohol
intake enjoy an 89% lower risk of colorectal cancer vs. CC or CT abstainers.
Conversely, high alcohol intake in TTers raises risk, more so than in their CC
or CT counterparts. High methionine intake is protective, but more so in
TTers. TTers have more trouble generating methionine, and are thus more
susceptible to the negative effects of alcohol or sub-optimal methionine intake
This
set of graphics takes our analysis a step further. Alcohol blocks several Methyl
Cycle enzymes (especially MTR which utilizes methyl-folate to remethylate
homocysteine back in to methionine). TT individuals with low alcohol
intake enjoy an 89% lower risk of colorectal cancer vs. CC or CT abstainers.
Conversely, high alcohol intake in TTers raises risk, more so than in their CC
or CT counterparts. High methionine intake is protective, but more so in
TTers. TTers have more trouble generating methionine, and are thus more
susceptible to the negative effects of alcohol or sub-optimal methionine intake
 On
the left, you can see that we TTers also have more to gain from high folate
intake. We have trouble converting folate in to methyl-folate so we
benefit more from high folate intake than do our CC and CT counterparts.
On
the left, you can see that we TTers also have more to gain from high folate
intake. We have trouble converting folate in to methyl-folate so we
benefit more from high folate intake than do our CC and CT counterparts.
Putting this together, TT status spares Methylene THF for DNA synthesis. It prevents us from robbing Peter (DNA generation) to pay Paul (generating glutathione and other Methyl Cycle products). TT status also leaves us more susceptible to the deleterious effects of Methyl Cycle toxins (alcohol and mercury) or suboptimal nutrient intake (folate and methionine). However, if we eat well and limit toxin exposure, we enjoy a reduced risk of malignancy. If we eat poorly and experience toxin exposure, we are at greater risk. If our Mothers eat poorly and/or harbor toxins, we are less likely to survive gestation. As Mothers are now eating better and supplementing with B Vitamins during pregnancy, more of us MTHFR TTs are making it through gestation. I could carry out a similar analysis on the other Methyl Cycle variants. These are all switches on Mother Nature's railroad tracks, designed to give Mankind the best opportunity to thrive under different environmental/food availability conditions. Whether this is the work of Our Creator or the product of four million years of Darwinian Evolution I will leave for you to decide. One more thing. Being TT renders one more susceptible to the Methyl Cycle depressant effects of alcohol, but this can be ameliorated by Methyl Cycle nutritional support, so for you we have designed high folate, high methionine beer (a little Methyl cycle humor)!
 A note about the RDA (US Government Recommended Daily Allowance) for folate and
other nutrients. The graphic on the left comes from a study whereby 60
healthy, 18-55 year old Mexican-American men, 1/2 CC (wild type, normal
function) and 1/2 TT (reduced function status, like me) were asked to transition
from their usual, self-selected diet to a diet that contained the RDA (438
mcg/day) of folic acid. Those with normal MTHFR function did just fine;
their homocysteine levels were normal at baseline and did not budge. Look
what happened to the TTers. Their self-selected diets were likely quite
adequate in folate and riboflavin, as despite TT status their mean homocysteine
level was normal at 11.5. On the low folate, RDA diet (what dieticians and
health care organizations are encouraged to recommend), homocysteine tripled to
a level that would dramatically increase their risk of multiple disease states.
A note about the RDA (US Government Recommended Daily Allowance) for folate and
other nutrients. The graphic on the left comes from a study whereby 60
healthy, 18-55 year old Mexican-American men, 1/2 CC (wild type, normal
function) and 1/2 TT (reduced function status, like me) were asked to transition
from their usual, self-selected diet to a diet that contained the RDA (438
mcg/day) of folic acid. Those with normal MTHFR function did just fine;
their homocysteine levels were normal at baseline and did not budge. Look
what happened to the TTers. Their self-selected diets were likely quite
adequate in folate and riboflavin, as despite TT status their mean homocysteine
level was normal at 11.5. On the low folate, RDA diet (what dieticians and
health care organizations are encouraged to recommend), homocysteine tripled to
a level that would dramatically increase their risk of multiple disease states.
As a TTer, I use this study as another reason not to trust government agencies. Humor aside, the whole concept of a RDA, a one size fits all for any given nutrient, is faulty. We vary so much in our genomic make up and in our conditional demand for different nutrients (due to acquired disease states or metabolic conditions) that applying RDA standards is inappropriate. I encourage all of my patients to undergo nutritional adequacy testing, and we then adjust your program to optimize your individual nutritional status.
James C. Roberts MD, FACC, FAARFM 3/5/16
SHMT C1420T:
Serine Hydroxy Methyl Transferase
Many Methyl Cycle diagrams indicate that
MTHFR converts THF (obtained from dietary or supplemental folic acid)
in to 5-methyl folate, which is then used by MTR to remethylate homocysteine in to
methionine, in the process regenerating THF. The diagram to the left
describes a key intermediate step, whereby P-5-P (activated form of B6)
dependent SHMT (Serine Hydroxy Methyl Transferase) transfers a methyl group from
the amino acid serine to form 5,10-methylene THF and glycine. You can see
that 5,10-methylene THF is not just the starting material for methyl-folate
generation; it is also necessary to generate pyrimidine and purine bases for new
DNA and RNA formation. Stated otherwise, without adequate 5,10-methylene
THF, not only are we unable to generate methyl-folate and SAMe, we also are
unable to repair or replicate our genetic template. Mother Nature's reason for
creating the MTHFR reduced function alleles, as discussed above, is to prevent
undue shunting of 5,10-methylene THF away from DNA repair. This is why
MTHFR 677TT individuals who eat as Mother Nature directs (or who make up for
poor diet with balanced supplementation) enjoy a reduced risk of colorectal
malignancy.
The equations below describe
how different enzymes convert 5,10-methylene THF in to different folate taxi
molecules (remember, folate molecules are just transport vehicles for methyl
groups derived from dietary serine, choline, and methionine).
MTHFD will be discussed in a different section. Thymidine Synthase transfers a methyl group from 5,10-methylene THF to dUMP (precursor of Uracil, a component of RNA) to form up dTMP (precursor of Thymidine, a component of DNA). If SHMT is not working optimally (1420 C ® T polymorphism, which some of you bear), or if dietary folate is inadequate or if upstream folate processing is impaired (discussed in a different section) then Thymidine generation will be impaired and we wind up making a mistake, incorporating Uracil in to DNA as opposed to Thymidine. We all do this a little, and many of us make this mistake more than a little, and if we do it a lot we develop a malignancy. Think of Uracil misincorporation in to DNA as you would an abnormal PAP smear or a precancerous skin lesion. If the misincorporation rate is low, we can easily repair the damage, but if the misincorporation burden is heavy, our attempts to repair the DNA lead to DNA fragmentation.

Individuals with low folate status demonstrate a 10-fold
increase in DNA Uracil misincorporation as compared
to those with adequate folate nutriture.
Supplementation resolves this error (why
folic acid may normalize an abnormal PAP smear). The graphic below
describes the effect of folate
supplementation on DNA Uracil misincorporation in a patient
with Crohn's disease and initially very poor folate
nutritional status. 
I don't know about you, but this concept of misincorporating Uracil in to DNA does not appeal to me. This will occur if folate intake or up stream folate processing is impaired. It is also more likely to occur if you are +/+ or +/- for SHMT C1420T. Here SHMT is not functionless, it is just sluggish. We address this allele by making sure that folate intake is adequate, and we also supplement you with the end products derived from 5,10-methylene THF, which you are having trouble making. Thus we supplement you with methyl-folate (at dose commensurate with your MTHFR status) and folinic acid. Folinic acid can cycle between the forms needed for DNA generation and THF. 400-800 mcg/day is usually recommended. CBS also uses serine as a methyl donor and CBS is also P-5-P dependent. Individuals with CBS up regulations (and BHMT down regulations) will often become serine and P-5-P deficient. We can assess your seine and P-5-P status with NutrEval testing and supplement you accordingly.
James C. Roberts MD, FACC, FAARFM 3/5/16
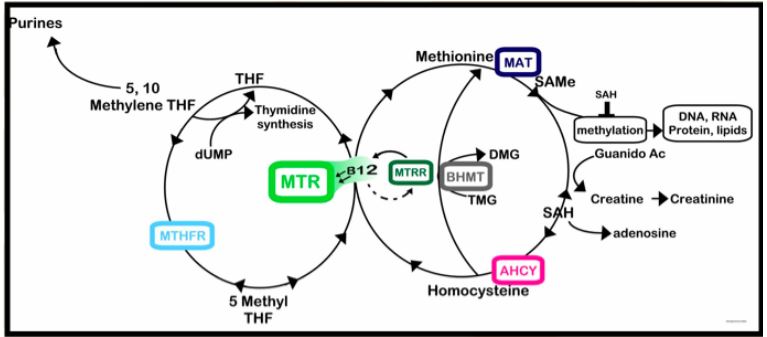
MTR combines 5-methyl folate and homocysteine to form methionine and tetrahydrofolate (THF). More specifically, MTR removes a methyl group from 5-methyl folate, then tacks it on to homocysteine to form methionine. In the process 5-methyl folate is converted back to THF.
The MTR A2756G defect is an up regulation. The enzyme is always on, grabbing every homocysteine and 5-methyl folate molecule that it can get its hands on, processing them to methionine and THF. Methyl-B12 is required for normal function of MTR, and with each spin of the MTR enzyme, one molecule of methyl-B12 is degraded and one molecule of methyl-folate is converted back to tetrahydrofolate (THF). The MTR up regulation thus creates the potential for methyl-folate and methyl-B12 deficiency. Should this occur, even the up regulated MTR enzyme will not be able to remethylate homocysteine (as it has no methyl-folate and methyl-B12 to work with - it wasted them). Homocysteine remethylation to methionine is compromised, SAMe is not formed, and thus systemic methylation fails.
Individuals +/- or +/+ for MTR A2756G defect often (but not always) will benefit form additional methyl-folate and methyl-B12 supplementation. Results of NutrEval (which assesses folate and B12 nutriture) and Drs. Data Methylation Panel (which gives us SAMe, SAH, and homocysteine) testing will guide us as to how much supplementation is optimal for you. When MTR is dysfunctional, to some degree we can bypass this step by supporting direct remethylation of homocysteine to methionine via the SHMT pathway (discussed later).
James C. Roberts MD, FACC, FAARFM 3/5/16
MTRR: Methionine Synthase Reductase
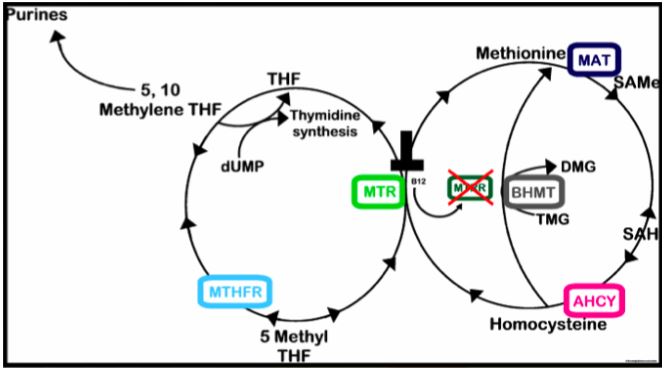
MTRR generates the methyl-B12 needed by MTR and many other methyl-B12 requiring enzymes. Blood B-12 levels may be normal, but if MTRR is (+/+) or (+/-), methyl-B12 formation will be compromised, homocysteine levels will be elevated, methylation in general will be compromised, and your physiology will be compromised.
MTR Up Regulation (+) and MTRR Down Regulation (+)
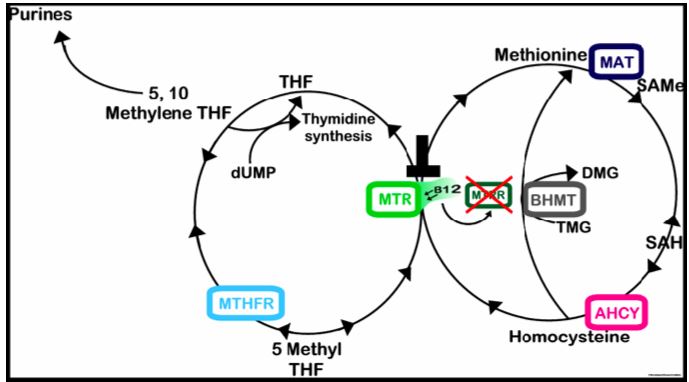
This combination leads to a double whammy on methyl-B12. You can’t make much because MTRR is not functioning well, and any methyl-B12 that you do make gets sucked up by the overactive MTR. Here the need to supplement with methyl-B12 (or to help you make it on your own) is greatest. You’d think that the treatment would be straight forward – give the patient methyl-B12. But remember, this is the Methyl Cycle that we are talking about, the most convoluted, conflicting, and therapeutically confusing physiologic system in the body.
We will talk about COMT a little later. COMT degrades dopamine, in the process using up methyl groups. Individuals who are COMT (+/+) degrade dopamine slowly. SAMe is a co-factor in the generation of dopamine, norepinephrine, and serotonin. Methyl-B12 and methyl donor supplementation in general may lead to an increase is neurotransmitter generation. Thus if we supplement COMT +/+ individual with excessive methyl-B12, TMG, or other methyl donors, we could potentially create an imbalanced state, with more dopamine and norepinephrine then COMT can neutralize, producing agitation and irritability. COMT (-/-) individuals need and tolerate methyl donors quite well. So if you are (+) for the MTR up regulation and/or (+) for the MTRR down regulation, and you are also COMT (-/-), all we need to do is to give you methyl-B12. We are giving you the methyl-B12 that you need, and any extra methyl groups left over can be put to good use. Conversely, if you are COMT (+/+), we will need to be cautious with respect to B12 supplementation. We will start with hydroxy-B12, expecting it to combine with the methyl groups available to form the methyl-B12 you need (the MTRR SNIPS do not code for absent MTRR function but rather for sluggish MTRR function, which we can likely overcome with enough hydroxy-B12). Later we may cautiously add in methyl-B12, backing down on the hydroxy-B12 dose, aiming to increase SAMe generation without producing irritability. This will be a step-by-step process, guided by laboratory testing (if methionine or SAMe are low then we need to push further here; if the values are OK then pushing with methyl-B12 is not necessary). B12 is reasonably well absorbed orally or via the sublingual route, and we can also administer it by injection, depending upon your individual needs and preferences. Now let’s move on to the previously alluded BHMT “backdoor” reaction.
James C. Roberts MD, FACC, FAARFM 3/5/16
BHMT: Betaine-Homocysteine Methyltransferase
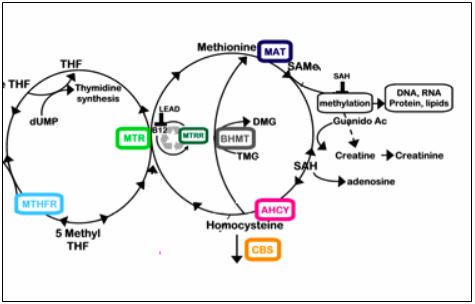 BHMT converts homocysteine directly in to methionine.
Specifically it removes a methyl group from TMG (trimethylglycine) and tacks it
on to homocysteine to form methionine and DMG (dimethylglycine). Stimulating a
genetically normal BHMT system will partially ameliorate the adverse affects of
other Methyl Cycle challenges. For example, if we cannot convert homocysteine
in to methionine because a MTHFR defect renders us deficient in methyl-folate,
or because an MTR up regulation or MTRR down regulation leaves us short in
methyl-B12, we can bypass these blockages by stimulating BHMT to
convert homocysteine directly in to methionine (I know this is difficult, but
bypassing blocked enzymes sure beats surgery to bypass blocked arteries, so
please read on). Our approach to BHMT, if it is defective, or when we want to
stimulate BHMT to help bypass MTR/MTRR defects, or when we want to pull
homocysteine away from a CBS up regulation, will be affected, to some degree, by your
clinical and COMT (basic
need for and tolerance to methyl group donors) status. The basic approach is as
follows:
BHMT converts homocysteine directly in to methionine.
Specifically it removes a methyl group from TMG (trimethylglycine) and tacks it
on to homocysteine to form methionine and DMG (dimethylglycine). Stimulating a
genetically normal BHMT system will partially ameliorate the adverse affects of
other Methyl Cycle challenges. For example, if we cannot convert homocysteine
in to methionine because a MTHFR defect renders us deficient in methyl-folate,
or because an MTR up regulation or MTRR down regulation leaves us short in
methyl-B12, we can bypass these blockages by stimulating BHMT to
convert homocysteine directly in to methionine (I know this is difficult, but
bypassing blocked enzymes sure beats surgery to bypass blocked arteries, so
please read on). Our approach to BHMT, if it is defective, or when we want to
stimulate BHMT to help bypass MTR/MTRR defects, or when we want to pull
homocysteine away from a CBS up regulation, will be affected, to some degree, by your
clinical and COMT (basic
need for and tolerance to methyl group donors) status. The basic approach is as
follows:
1. Trimethylglycine (Betaine) will stimulate BHMT and
will lower homocysteine. The graphics below show the affect of increasing
doses of supplemental TMG (Betaine) on fasting and post-methionine loading
homocysteine values over six weeks. Note that baseline post-methionine
homocysteine is three-fold greater than the corresponding fasting value. A
methionine load leads to SAMe generation, SAMe usage to generate SAH, which will
then be rapidly converted in to homocysteine. Methionine loading can be
considered a stress test of the Methyl Cycle, and also mimics what is happening
in your physiology after a high protein meal. One caveat here, TMG does
provide methyl groups, and COMT + individuals may experience irritability with
excessive methyl donor supplementation. Fibrate lipid lowering agents
(Fenofibrate but not Gemfibrozil) deplete TMG and increase homocysteine,
particularly in diabetics, who tend to be low in TMG.
2. Zinc is necessary for proper BHMT function; here we can
supplement you with Zinc 25 mg/day or as indicated by the results of nutritional
testing (24 hour urine mineral or NutrEval assessment).
3. Phophoserine (which we also use to modulate elevated
cortisol) can be converted in to TMG and will stimulate BHMT.
4. Phosphatidylcholine is discussed in more detail within the Methyl Thieves
section, but can also be converted in to TMG and will stimulate BHMT and lower
homocysteine.
5. DMG (dimethylglycine) will inhibit BHMT activity and is best replaced by TMG
when an increase in homocysteine remethylation via the BHMT pathway is desired.
James C. Roberts MD, FACC, FAARFM 3/5/16
COMT: Catechol–O–Methyl Transferase
COMT (Catechol-O-Methyl Transferase) is a Phase Two Biotransformation enzyme that inactivates catecholamines, estrogen molecules, and bioflavonoid nutrients. COMT transfers a methyl (-CH3) group from SAMe to the catechol group (HO-C=C-OH) of the catechol molecule being processed, changing its chemical structure and chemical properties. Our body processes endogenous and toxic molecules in a step-by-step process. Phase One enzymes activate a molecule/toxin, typically to a more biologically active (and potentially more toxic) form. Phase Two enzymes such as COMT add a "clearance" group (in this case a methyl group) to the activated substance, neutralizing it and/or rendering it more amenable to excretion via the Phase Three liver, GI tract, and kidneys.
COMT is a "low specificity" and "high capacity"
biotransformation enzyme. Some enzymes act on only one molecules
(e.g. Superoxide Dismutase 2 acts only on Superoxide within the mitochondria)). COMT is not specific;
it will O-Methylate
any molecule that contain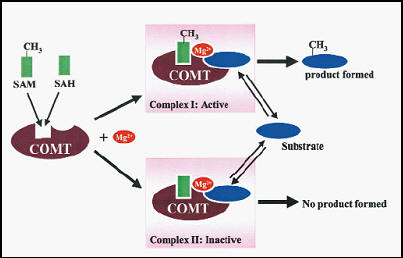 s a catechol group. As a high
capacity system, it is not easily overwhelmed. You can throw large
quantities of estrogen molecules (estradiol and estrone), catecholamines
(dopamine, norepinephrine, and epinephrine), and bioflavonoids (quercetin and
the polyphenols found in coffee and tea), at COMT and COMT can O-Methylate
all of them. Wild type (genomically normal) COMT is never the rate
limiting step. However, SAH (S-Adenosylhomocysteine) is. COMT has
two binding sites. One (the active site) binds to SAMe, the second (the
catalytic site) binds to the catechol substrate and magnesium. COMT then
transfers a -CH3 group from SAMe to the catechol target, forming a methylated
product and SAH (S-Adenosylhomocysteine). As you are aware, whenever we
"spend" a SAMe, we generate a SAH. While SAMe activates COMT, SAH inhibits
it. SAMe binds the active site on COMT, but SAH binds it more avidly.
The rate limiting step in COMT methylation is SAH accumulation, with a resulting
low, and thus ineffective, SAMe:SAH ratio. Under normal circumstances, SAH
is rapidly converted in to homocysteine, SAH is kept low, the SAMe:SAH ratio is
kept high, and COMT can methylate all it wants. However, when Methyl Cycle
genomic or nutritional abnormalities result in homocysteine elevation, SAH
cannot be cleared to homocysteine (the process backs up), and COMT activity shuts down.
Genomically impaired COMT is a problem. Elevated homocysteine/SAH is a
problem. Impaired COMT plus elevated homocysteine/SAH is a metabolic
disaster. Disruption in catecholamine degradation is the primary link
between high homocysteine and atherosclerosis!
s a catechol group. As a high
capacity system, it is not easily overwhelmed. You can throw large
quantities of estrogen molecules (estradiol and estrone), catecholamines
(dopamine, norepinephrine, and epinephrine), and bioflavonoids (quercetin and
the polyphenols found in coffee and tea), at COMT and COMT can O-Methylate
all of them. Wild type (genomically normal) COMT is never the rate
limiting step. However, SAH (S-Adenosylhomocysteine) is. COMT has
two binding sites. One (the active site) binds to SAMe, the second (the
catalytic site) binds to the catechol substrate and magnesium. COMT then
transfers a -CH3 group from SAMe to the catechol target, forming a methylated
product and SAH (S-Adenosylhomocysteine). As you are aware, whenever we
"spend" a SAMe, we generate a SAH. While SAMe activates COMT, SAH inhibits
it. SAMe binds the active site on COMT, but SAH binds it more avidly.
The rate limiting step in COMT methylation is SAH accumulation, with a resulting
low, and thus ineffective, SAMe:SAH ratio. Under normal circumstances, SAH
is rapidly converted in to homocysteine, SAH is kept low, the SAMe:SAH ratio is
kept high, and COMT can methylate all it wants. However, when Methyl Cycle
genomic or nutritional abnormalities result in homocysteine elevation, SAH
cannot be cleared to homocysteine (the process backs up), and COMT activity shuts down.
Genomically impaired COMT is a problem. Elevated homocysteine/SAH is a
problem. Impaired COMT plus elevated homocysteine/SAH is a metabolic
disaster. Disruption in catecholamine degradation is the primary link
between high homocysteine and atherosclerosis!
Let's study COMT and its relationship to CV disease.
Let's say you require open heart surgery. As a major procedure, open heart
surgery is associated with the sustained release of catecholamine (sympathetic
nervous system, "fight or flight) neurotransmitters, such as norepinephrine,
dopamine, and epinephrine. While elevated, these chemicals constrict blood
vessels, reduce kidney blood flow, strain the heart, and promote arrhythmia.
Fortunately, COMT (when functionally normally) can break them down, reversing
these effects, all of which are undesirable in the post-op patient. What would
happen if 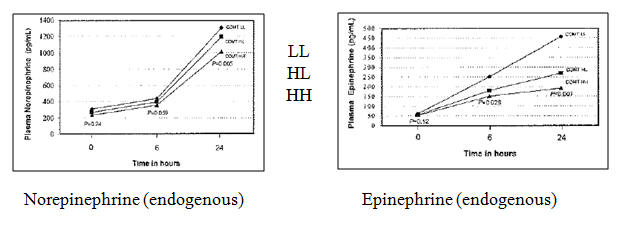
COMT was hypofuncitonal? In this study, individuals homozygous for reduced function COMT (designated LL, for Low-Low, on the charts), homozygous for normally functioning COMT (HH), and heterozygous individuals (HL) all underwent open heart surgery. The physicians involved were unaware of the genotypes of the patients and thus no genotype-specific care was provided. As you would predict, the COMT-LL group had trouble handling the catecholamine surge of surgery. Their post-op epinephrine and norepinephrine levels were higher. They required greater doses of diuretic (furosemide) therapy, were more likely to experience kidney dysfunction and shock, and mortality was greater. 5% of the COMT-LL patients died in the hospital and another 6% passed away within the first 6 months post-op. None of the COMT-HH patients died! COMT is important. Adequate function of the Methyl Cycle is important. If this study were to be repeated and homocysteine status included, my hunch is that the highest death rate would occur in COMT-LL individuals with elevated homocysteine.
Is coffee good or bad for you? Coffee provides beneficial bioflavonoid antioxidants. Coffee also provides caffeine, which releases catecholamines. If COMT is functioning normally, heavy coffee intake is associated with a reduced risk of CV disease. If COMT is dysfunctional, you can't break down the catecholamines, and chronic catecholamine overload ensues. The vascular toxicity of chronic catecholamine overload outweighs the benefits of the bioflavonoids and CV risk increases (if you are +/+ for CYP1A2, which breaks down caffeine, your high coffee/poor COMT function risk would be further increased.
As stated above, when SAH is elevated, such that the SAMe:SAH is low, then COMT becomes dysfunctional. We rely on COMT to methylate the "neutral" 2-OH Estradiol to the anti-malignancy, anti-cancer molecule 2-methoxyestradiol. Here we see (in a laboratory setting) that as the level of 2-OH Estradiol increases, COMT generates increasing levels of 2-methoxyestradiol. Conversely, with increasing levels of SAH, 2-methoxyestradiol generation from 2-OH Estradiol declines. This is one of the links between elevated homocysteine (which leads to elevated SAH and a low SAMe:SAH) and increased risk of reproductive organ malignancy.
Let's now look at the interaction between genomic COMT dysfunction, poor folate status, elevated homocysteine, and future cardiovascular risk. 792 healthy Finnish men were followed for nine years and over this time period 69 experienced a cardiac event. Baseline homocysteine was a little higher and folate a little lower in those who went on to experience an event.
If your were in the lowest tercile
(lowest 1/3rd) for folate, your risk increased by 70%. If you were in the
upper tercile for homocysteine, your risk increased by 40%. 28% were
homozygous for reduced COMT function, and their risk was increased by 70%.

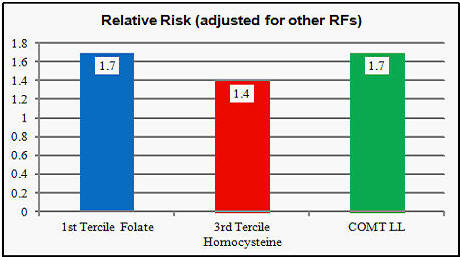
The charts below show that risk associated with high homocysteine or low folate is increased in the presence of genomic COMT dysfunction.
Risk is lowest if homocysteine is low and COMT function OK (-/- or +/-). If homocysteine is high but COMT intact, risk rises by 15%, as the elevation in homocysteine will compromise COMT function even if COMT is not genomically impaired. Even if homocysteine is low, if COMT function is poor (+/+), catecholamines can not be broken down, and risk increases, in this study by 40%. With the double whammy of high homocysteine and poor COMT function, risk rises 2.6 fold, reflecting extremely compromised catecholamine clearance.
Risk if low when folate is high and COMT function intact. Low folate will compromise SAMe generation, and without adequate SAMe even genomically intact COMT cannot break down catecholamines, and thus risk rises nearly two-fold. If folate is high but COMT function impaired, likewise catecholamines can not be cleared and risk rises just over two-fold. Risk rises 2.7-fold when folate is low and COMT activity is impaired.
Individuals with genomic or acquired COMT dysfunction are at greater risk when the SAME:SAH ratio is low, and the most important cause of low SAMe:SAH is elevated homocysteine. Thus is your COMT function is genomically compromised it is critical that we keep your homocysteine level within the physiologic range.
The V158M and H62H alleles of COMT are down regulations, associated with sluggish COMT function. Individuals (+/+) or (+/-) for these genes will degrade dopamine only slowly. Now, while COMT (+) status is not the norm, from our perspective it is not always a bad thing. Dr. Yasko feels that we need dopamine to defend against microbes and heavy metals; here being (+) for COMT is actually in our favor. While genomic COMT dysfunction increases cardiovascular risk, the attendant reduction in catecholamine clearance may have favorable effects on mood. Dopamine gives us drive and get-up-and-go. Thus COMT +/+ individuals are at lower risk of depression in comparison to COMT -/- individuals who can clear dopamine rapidly. BH4 deficiency can occur as a consequence of oxidative stress or DHFR, GCH1, CBS, and possibly "backward” MTHFR A1298C SNIPs. We need BH4 to carry out multiple physiologic steps, including the generation of dopamine. If our COMT (+) status keeps us from breaking down dopamine, we do not need to “spend” BH4 to make dopamine, leaving more BH4 available for other critical functions.
Conversely, a potential downside of methyl donor
supplementation in an individual +/+ or +/- for a COMT down regulation is that
the methyl donors will generate ,ore dopamine and catecholamine
neurotransmitters that COMT can break down, leading to anxiety and agitation.
Here too many methyl groups can lead to mood swings. Panic
attacks and bi-polar mood disorder are seen with greater frequency in COMT (+)
individuals; this makes sense. COMT (-) individuals, on the other hand, need
and tolerate methyl groups. A third, and less frequently encountered COMT
abnormality, COMT 61, is an up regulation variant. Individuals (+) for COMT 61
breakdown dopamine quite rapidly and are at greatest need for methyl donors. To
summarize in chart form: 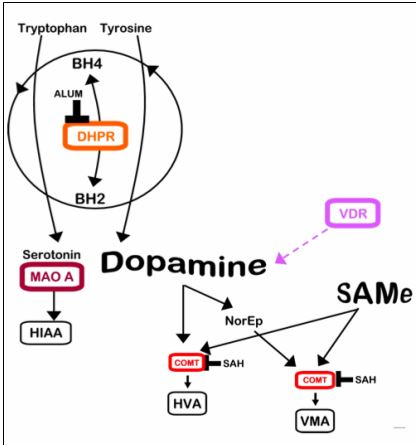
|
COMT H62H
(+/+) |
Highest
dopamine levels |
|
COMT H62H
(-/-) |
Lowest dopamine
levels |
* I am COMT H62H and L136L (-/-), but my wife refuses to believe this!
Dopamine levels as they relate to our COMT
status will also be affected by the VDR Taq gene,
which influences dopamine production in relation to Vitamin D.
Plan of action for COMT +/+ (and to a lesser extent for COMT +/-)
1.
Here it is critical that homocysteine is not elevated.
2. Ideally measure SAMe and SAH, and if the ratio is low take corrective action.
3. If COMT is +/+ and you are having trouble lowering SAH, you can cut back on
SAH generation by:
a. Limiting bioflavonoid intake (especially quercetin) as when these molecules
are methylated by COMT a SAMe is converted in to a SAH.
b. Limit estrogen supplementation, as when hydroxy-estrogen molecules are
methylated by COMT, likewise SAMe is converted in to SAH.
c. Supplement with phosphatidylcholine and creatine, also to decrease SAMe
expenditure in to SAH (please see the Methyl Thieves section).
James C. Roberts MD, FACC, FAARFM 3/5/16
VDR Taq: Vitamin D Receptor Taq Abnormality
Vitamin D has many functions, an issue because 90% of my patients have low or low normal Vitamin D levels. Pertinent to this discussion, Vitamin D stimulate the enzymes that generate dopamine, a good reason to keep your Vitamin D level up, as we need dopamine to defend against microbes and metals, and to keep our mood up. While we utilize SAMe (and indirectly other methyl group donors) to degrade dopamine, we also utilize methyl donors to generate dopamine. Individuals with a normal Vitamin D receptor, those who are VDR Taq (-/-), make plenty of dopamine. They tend not to need or to tolerate methyl groups or dopamine precursor substances. With respect to methyl group need and tolerance, they behave like COMT (+) individuals. Individuals (+/+) or (+/-) for VDR Taq defect have lower Vitamin D levels, make less dopamine, and will need and tolerate dopamine precursor substances and methyl donors. With respect to methyl donor tolerance, VDR Taq (+) individuals behave like COMT (-) individuals. All sorts of permutations are possible here, impacting on your tolerance and need for dopamine precursors and methyl groups. I acknowledge that this is all very difficult to understand. Hopefully the chart below will help.
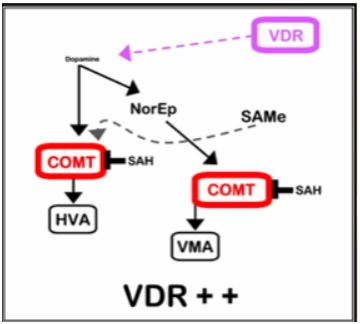
|
COMT (+/+) |
Highest
dopamine levels |
|
In such as individual, we would utilize the “un methylated” forms of Methyl Cycle intermediates. If an MTR/MTRR defect increases your need for methyl-B12, in this individual we would start with hydroxy-B12, to avoid ODing you with methyl groups, expecting that with enough hydroxy-B12 and free methyl groups floating around you will form up some methyl-B12, even if MTRR activity is compromised by a defect. We would not give your dopamine precursors such as quercetin or the herb macuna puriens. We would not advise a diet high in tyrosine, the amino acid precursor of dopamine. COMT (+/+) VDR Taq (-/-) individuals will be susceptible to iodine and lithium depletion as they detoxify, and we will have to watch for this and supplement accordingly. |
|
|
COMT (-/-) |
Lowest dopamine
levels |
|
In such an individual, we would utilize the methylated forms of Methyl Cycle intermediates, including methyl-B12 if n TR/MTRR defect is present. Dopamine precursors such as quercetin, ginkgo biloba, and the herb macuna puriens might be helpful, as would a diet high in tyrosine, the amino acid precursor to dopamine. Other methyl donors, including melatonin, TMG, turmeric, theanine, along with MSM and SAMe (the latter two only for CBS (-/-) individuals) would make sense. To support BHMT, instead of Phosphatidylserine, we would use Pedi-Activ, which contains Phosphatidylserine and DMAE, a methyl donor. Rather than using GABA to deal with excitotoxicity, we would use Zen, which combines GABA with the methyl donor threanine. |
|
|
COMT (+/-) and
VDR (-/-) behaves like COMT (+/+) |
|
|
Multiple (+/-) combinations of COMT and VDR Taq are possible. We will address these “intermediate” genotypes with intermediate levels of methyl group supplementation. I will be more specific on your individual report. |
|
Methyl Thieves and SAMe Stealers
A key goal of Methyl Cycle physiology (and a focus in our work with you) is to
ensure sufficient, replenishable, and physiologic (not excessive) supplies of:
A. SAMe, along with and an appropriate SAMe to SAH ratio (it is the ratio, not
just the SAMe level, that drives forward useful methylation reactions).
B. BH4 (needed to generate neurotransmitters and nitric oxide).
C. Key antioxidant and detoxification molecules (glutathione, taurine, sulfate,
and cysteine).
D. Purine and Pyrimidine bases for DNA and RNA generation.
You are generating (or taking) methyl folate and methyl B12, not for the sake of generating high levels of these Methyl Cycle intermediates (yes, intermediates, not finished products), but rather to help ensure that the Methyl Cycle work products (SAMe, BH4, glutathione, cysteine, and taurine) are in adequate supply.
While our focus has been on improving SAMe supply, we should also consider means to reduce SAMe expenditure (Mother Nature balances supply and demand – the government should pay heed)! Stated otherwise, if nutritional supplementation decreases demand for SAMe, more will be available to meet critical demands (e.g. DNA methylation to silence inflammatory and proto-oncogenes).
So how are we “spending” SAMe? What phenomena lead to SAMe wasting or diversion? How do we ameliorate these pathophysiologies to restore SAMe and appropriate SAMe:SAH balance?
In considering SAMe expenditure, remember that each time we “spend” a SAMe (S-Adenosylmethionine) to carry out a specific methylation reaction, we create a SAH (S-Adenosylhomocysteine), which in turn inhibits methylation. A declining SAMe:SAH inhibits methylation reactions; it does us no good to increase SAMe if at the same time we build up SAH.
Fortunately, SAH is rapidly converted to Homocysteine and Adenosine. Adenosine is efficiently removed, but if the Methyl Cycle is sluggish, due either to SNIPS, toxins, or nutritional deficiency, Homocysteine will build up. Homocysteine will then be back converted to SAH, the SAMe:SAH ratio falls, and useful methylation grinds to a halt. Homocysteine itself is not the problem; it is the buildup of SAH, compromising methylation potential, which leads to disease states such as atherosclerosis, cancer, and mood disorders.
So what processes “steal” SAMe? In considering this issue, we need to be aware that CBS (which irreversible drains Homocysteine down the trans-sulfuration pathway and away from SAMe reformation) is up regulated (enzymatic activity increases) by oxidative stress and inflammation.
A. Oxidative stress: When the generation of free radicals (superoxide, hydroxyl, and hydrogen peroxide) outpaces our ability to neutralize them with endogenous (e.g. superoxide dismutase) or exogenous (supplemental antioxidants), we suffers from a buildup of free radicals. To address this immediate threat to health, Homocysteine metabolism down the CBS pathway (irrespective of genomic status) will increase. Homocysteine (and with it the potential to create new SAMe) will be irreversibly diverted away from remethylation (via MTR and BHMT back into methionine for conversion to SAMe) and towards the production of glutathione, taurine, and cysteine.
This all makes sense. Oxidative stress damages our physiology and kills cells. When faced with oxidative death, it makes sense to divert Methyl Cycle resources towards antioxidant generation. After oxidative stress has been neutralized, CBS flow will decrease, Homocysteine will start flowing back towards SAMe, and useful methylation reactions will resume. Our problem is that most ill Americans suffer from unremitting oxidative stress (we can measure your individual level of oxidative stress with the NutrEval study). Homocysteine will thus be shunted down the CBS pathway, such that useful methylation of DNA, estrogen molecules, and catecholamines will be compromised. If you cannot methylate catecholamines, then oxidative stress will develop within your blood vessels. If you cannot methylate your DNA, than you cannot silence inflammatory genes. You thus make more inflammatory molecules, more free radicals build up, more Homocysteine is diverted away from SAMe regeneration, and you are now chronically ill.
The solution is to undergo an assessment of oxidative stress, and then takes steps to resolve any challenges present. This will involve removing from your body phenomena that generate free radicals (e.g. smoking, toxic metals, organic pollutants) while concomitantly shoring up your antioxidant defenses with nutrients that we find to be in short supply (selenium, Vitamin E, Vitamin C, etc.). We will apply the principles of nutritional medicine to help you generate SAMe and to prevent oxidative stress from “stealing” Homocysteine away from SAMe regeneration. As a side note, toxic metals not only “steal” SAMe, they also compromise its formation (e.g. Mercury compromises MTR, in this fashion blocking useful remethylation of Homocysteine back into methionine for conversion into SAMe).
Those of you with reduced function SNIPS for the major antioxidant defense enzymes (superoxide dismutase, catalase, glutathione peroxidase, and glutathione reductase) are genomically predisposed to oxidative stress. We can compensate for this. First we assess your antioxidant genotype, oxidative stress, and nutritional status. Then we take corrective action, removing radical generating toxins while supplementing with antioxidant vitamins, minerals, polyphenols, and a diet rich in fruits and vegetables. Then we repeat your metabolic assessment. We can get it right, and you can resolve chronic oxidative stress.
B. Inflammation: Inflammatory TH1/TH17 cytokines, such as TNF-alpha, Il-6, and Il-1b also increase flow down the CBS pathway, draining Homocysteine away from useful remethylation back in to SAMe. Inflammation leads to oxidative stress and oxidative stress leads to inflammation. Both are useful in fighting infection, but both processes are persistently elevated as our immune system misinterprets as infection the chronic “pseudoinfections” of visceral obesity, leaky gut, and environmental toxicity. Thus by resolving inflammation (either with anti-inflammatory nutrition interventions such as turmeric or berberine) or by removing the cause of chronic inflammation (weight loss or resolving leaky gut) we can resolve the “inflammatory drain” on SAMe supply and demand.
What processes deplete our SAMe stores? Are some less critical than others? Can we decrease SAMe demand with nutritional supplementation?
A. DNA methylation: This is sacrosanct. Only SAMe can methylate DNA. Only SAMe can shut down the transcription (reading into protein formation) of viral, inflammatory, and proto-oncogenes (promote cancerous transformation) while maintaining the transcription of tumor suppressing and anti-inflammatory genes. We can’t scrimp on DNA methylation, but by resolving oxidative/inflammatory stress, and supplementing with SAMe “sparers” (described below), we can maintain adequate SAMe (with a high SAMe:SAH ratio) to ensure optimal DNA methylation.
B. Creatine formation: Around 50% of our SAMe is “spent” in the generation of creatine, a molecule critical to energy maintenance. We do work by splitting a high energy bond within ATP (Adenosine Triphosphate) to produce ADP and phosphate. We burn carbon and use this energy to rephosphorylate ATP. When energy is plentiful, ATP will transfer a phosphorus group to creatine, forming Phosphocreatine. Should we suddenly run out of ATP energy (sprinting, weight lifting, or if oxygen supply:demand is compromised by a blocked artery or failing heart), Phosphocreatine can download a high energy phosphate bond back to ADP, regenerating ATP such that cellular work can continue. We actually store 10 heart beats of energy as Phosphocreatine. As you would expect, creatine supplementation has been shown to be helpful in anaerobic athletic performance as well as in heart failure. Of interest, creatine has been shown to lower cholesterol, and while the literature is not 100% consistent, creatine supplementation will decrease expenditure of SAMe and increase the SAMe:SAH ratio. Athletes take 5 grams of creatine, four times a day (saturation dose) for one week, followed by 5 grams/day (maintenance dose). However, unless you have an athletic competition coming up, you can simply add 5 grams of creatine/day to your program. Creatine is not unsafe, but there have been instances where competitive body builders dosed up on creatine while decreasing fluid intake (so their muscles will bulge out more) leading to dehydration and kidney compromise. Creatine is converted in to Creatinine, which is filtered out by the kidneys. We use serum creatinine to gauge kidney function. A trivial rise in serum creatine may occur when you supplement with creatine. This does not mean that kidney function is decreasing; rather this is an artifact due to creatine supplementation. Creatine supplementation at 5 grams/day makes sense for individuals with Methyl Cycle SNIPS that might compromise SAMe generation or maintenance (MTHFR, MTR, and BHMT), or when we feel that chronic oxidative/inflammatory stress is depleting SAMe regeneration.
C. Phosphatidylcholine: Three SAMe molecules, around 30% of our total supply, are used to methylate phosphoethanolamine into phosphatidylcholine. Phosphatidylcholine (PC) is involved in lipoprotein formation and reverse cholesterol transport; PC is also a critical component of the cell membrane. The common name for PC is lecithin. PC/lecithin is essentially a triglyceride like molecule with two fatty acids and one phosphocholine group attached to a three carbon glycerol backbone. The biochemical utility of PC relates to the composition of its two fatty acids. PC containing two unsaturated linoleic acid molecules (polyenylphosphatidylcholine) is used IV and orally to treat cardiovascular, liver, and neurological disease (see our DVD presentation). If we supplement you with PC, less SAMe will be spent generating PC, and more will be available for useful methylation reactions. In addition, the less SAMe spent, the less SAH and Homocysteine will be formed. Furthermore, PC can be converted into choline, which can be converted into Betaine (TMG or trimethylglycine) which is used by BHMT to directly remethylated homocysteine back in to methionine (which is then converted in to SAMe). Thus PC supplementation will lower an elevated Homocysteine and increase SAMe supply along with the SAMe:SAH ratio. We use PhosChol (unsaturated phosphatidylcholine rich in linoleic acid) 900 to 2700 mg/day in the treatment of cardiovascular and liver disease. Our dose in Methyl Cycle patients will relate to your SNIP status and baseline Homocysteine level.
D. COMT utilization. COMT (Catechol-O-Methyl transferase) metabolizes estrogen molecules, catecholamines (dopamine and norepinephrine), drugs (e.g. L-Dopa used in the treatment of Parkinson’s disease) and bioflavonoids (particularly Quercetin) by transferring a methyl group from SAMe to an oxygen molecule on the compound being methylated. Each time this occurs, SAH is generated, the SAMe:SAH ratio falls, and COMT and all other methyl-transferase enzymes are inhibited. If we are interested in sparing SAMe and maintaining a high SAMe;SAH ratio, it would be prudent to reduce the need for COMT-driven methylation. Lowering stress will lower norepinephrine, and thus decrease SAMe utilization by COMT. While bioflavonoids such as Quercetin have many beneficial properties, if SAMe preservation is critical (high Homocysteine in the presence of MTHFR, MTR, MTRR, and BHMT SNIPs or if our ability to methylate estrogen molecules is impaired) then decreasing intake of Quercetin and related bioflavonoids would be prudent. Conversely, when insufficient dopamine is the problem, we might use Quercetin to blunt dopamine degradation by “clogging up” COMT. Caffeine increases catecholamine production. Caffeine intolerant individuals are typically COMT +. When caffeine intolerance develops anew, we look for new problems that might be compromising SAMe supply or COMT functionality.
E. Drug effects. Many prescription and over the counter agents compromise Methyl Cycle function, leading to important (but initially silent) long-term side-effects. “Purple Pills” for reflux and stomach upset blunt B Vitamin absorption, increasing homocysteine. Oral contraceptives, metformin, non-spironolactone diuretics, alcohol, toxins in general, and many seizure meds compromise B Vitamin metabolism and/or Methyl Cycle function. Niacin uses up a great deal of SAMe in its metabolism and compromises recycling of B6. You can see this in a rising homocysteine level. Beta-Blockers actually lower homocysteine, as do Fish Oil and N-Acetyl Cysteine. Statin drugs have no effect; Fenofibrate will increase homocysteine while gemfibrozil does not. Some of these drugs are critical for other aspects of your health. We understand how these drugs compromise B Vitamin metabolism and we can take corrective action; you thus get the benefit of the therapeutic agent without the Methyl Cycle dysfunction downside.
Plan of action for Methyl Thieves and SAMe Stealers )
(made out of context of your MTHFR, MTR, MTRR, COMT, VDR, and personal health
status)
1. Evaluate for the presence of oxidative and/or inflammatory stress and take
corrective action. A Genova Labs NutrEval study will be quite helpful in this
regard.
2. Creatine 5 grams/day (mixed in a liquid) to spare SAMe.
3. PhosChol, 900-2700 mg/day, to spare SAMe and promote homocysteine
methylation.
4. Discontinue (or compensate for nutritionally) any drugs you are receiving
that cause Methyl Cycle dysfunction.
James C. Roberts MD, FACC, FAARFM 5/25/15
MTHFR A1298C: 5,10-MethyleneTetraHydroFolate Reductase (Þ BH4)
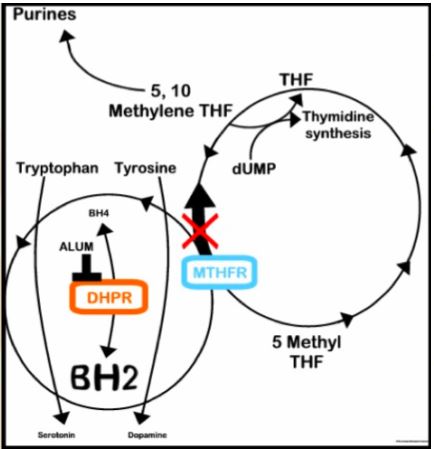
The MTHFR C677T polymorphism effects the “forward reaction”, the
conversion of THF in to 5-methyl folate. MTHFR A1298C has less of an
adverse effect on forward
5-methyl folate production. It is Dr. Yasko's position that the MTHFR
reaction is reversible, that MTHFR can convert methyl-folate back in to
5,10-methylene tetrahydrofolate, in the process recycling "spent" BH2 back in to
useful BH4. I cannot corroborate this position in the literature, and I
have looked. Other authors talk about it,
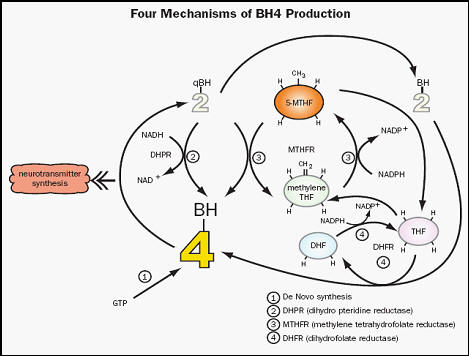 but no proof is available. This
doesn't mean that Dr. Yasko is wrong; rather it means that I cannot back up this
position. However, there is a pathway through which methyl-folate will
regenerate BH4. MTR removes the methyl group from methyl-folate as it
remethylates homocysteine back in to methionine, generating raw material THF.
In the folate processing section we will talk a little more about DHF
(Dihydrofolate Reductase). DHF converts oxidized folate molecules to DHF
and then in to useful THF, and this reaction is reversible. High levels of
methyl-folate will favor this reverse reaction, and in the process BH2 is
recycled back to BH4. Also, Methyl-folate looks a lot like BH4. With
respect to eNOS (endothelial nitric oxide synthase) function, methyl-folate
enhances binding between eNOS and BH4, and when BH4 is in short supply,
methyl-folate can "stand in" for BH4. Whether A1298C affects BH4 recycling
or not, strong methyl-folate status will lead to strong BH4 status, a desirable
state of affairs. We often need help with respect to BH4 recycling. The
enzyme DHPR recycles BH2 back in to BH4. DHPR is sensitive to toxins (mercury,
lead, and particularly aluminum). Oxidative stress (superoxide and
peroxynitrite in particular) degrade BH4, and we also use up BH4 dealing with
ammonia generated when the CBS pathway is unregulated. Methyl-folate
improves endothelial function and we are quite liberal with its use in the
treatment of cardiovascular conditions.
but no proof is available. This
doesn't mean that Dr. Yasko is wrong; rather it means that I cannot back up this
position. However, there is a pathway through which methyl-folate will
regenerate BH4. MTR removes the methyl group from methyl-folate as it
remethylates homocysteine back in to methionine, generating raw material THF.
In the folate processing section we will talk a little more about DHF
(Dihydrofolate Reductase). DHF converts oxidized folate molecules to DHF
and then in to useful THF, and this reaction is reversible. High levels of
methyl-folate will favor this reverse reaction, and in the process BH2 is
recycled back to BH4. Also, Methyl-folate looks a lot like BH4. With
respect to eNOS (endothelial nitric oxide synthase) function, methyl-folate
enhances binding between eNOS and BH4, and when BH4 is in short supply,
methyl-folate can "stand in" for BH4. Whether A1298C affects BH4 recycling
or not, strong methyl-folate status will lead to strong BH4 status, a desirable
state of affairs. We often need help with respect to BH4 recycling. The
enzyme DHPR recycles BH2 back in to BH4. DHPR is sensitive to toxins (mercury,
lead, and particularly aluminum). Oxidative stress (superoxide and
peroxynitrite in particular) degrade BH4, and we also use up BH4 dealing with
ammonia generated when the CBS pathway is unregulated. Methyl-folate
improves endothelial function and we are quite liberal with its use in the
treatment of cardiovascular conditions.
James C. Roberts MD, FACC, FAARFM 5/25/15
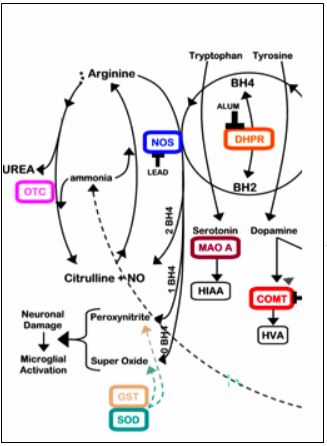
In a BH4 dependent reaction, Nitric Oxide Synthase (NOS)
converts Arginine in to Nitric Oxide, the molecule that resists plaque
formation, vasospasm, and abnormal clotting. If you can make and maintain
Nitric Oxide then you will not develop cardiovascular disease. If you have
cardiovascular disease and if we can successfully reboot your Nitric Oxide
system, than we can stabilize your disease. Every maneuver in drug and non-drug
cardiovascular medicine that improves patient symptomatic status and outcome
works on this system. Every risk factor (or causative factor for cardiovascular
disease) compromises Nitric Oxide generation or maintenance. NOS is also
involved in ammonia detoxification, a job that distracts it from its Nitric
Oxide generating duties and which uses up BH4. Without adequate levels of BH4
Nitric Oxide Synthase will not convert Arginine in to beneficial Nitric Oxide,
but rather in to undesirable free radical species such as superoxide or
peroxynitrite.
The NOS D298E abnormality codes for a dysfunctional NOS enzyme. It has trouble breaking down ammonia and it has trouble generating Nitric Oxide. NOS (+) individuals are at greater risk for developing all forms of cardiovascular disease, for experiencing adverse events, and for restenosis following balloon angioplasty. A component of “a positive family history of cardiovascular disease” is related to genes coding for high cholesterol, elevated lipoprotein (a), and iron over absorption. The rest likely relates to inherited abnormalities in NOS, ACE, and the other Methyl Cycle genes. If you are NOS (+) we will pay particular attention to maneuvers designed to lower your ammonia burden, and to address risk factors that compromise Nitric Oxide. As the products of a compromised or genetically abnormal NOS system are the free radicals superoxide and peroxynitrite, aggressive antioxidant supplementation makes sense here (while a broad spectrum program of antioxidant supplementation is always wise, we specifically use Vitamin C to neutralize superoxide and 5-methyl folate to neutralize peroxynitrite). I give two separate two hour presentations on Endothelial Dysfunction, which we have on cassette tape (we will likely have a DVD presentation available late next fall). BH4 supplementation has been demonstrated to improve Nitric Oxide generation and endothelial function in individuals with risk factors such as hyperlipidemia, and we presume that it will do the same in individuals with Methyl Cycle abnormalities.
ACE: Angiotensin Converting Enzyme
Angiotensin Converting Enzyme (ACE) converts Angiotensin I,
a weak vasoconstrictor, into Angiotensin II, for our purposes a nasty
angiochemical that mediates hypertension, plaque deposition, salt and water
retention, magnesium and potassium wasting, and abnormal clotting. ACEI (angiotensin 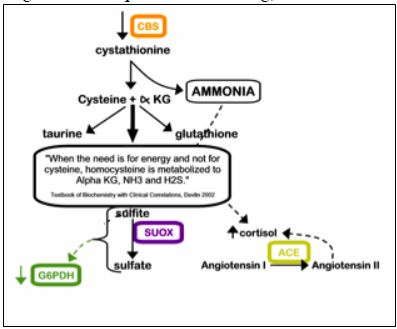 converting
enzyme inhibitors) target this enzyme, seeking to block generation of
Angiotensin II. The potassium and magnesium sparing diuretic Spironolactone
blocks the deleterious effects of Aldosterone, another mediator that is up
regulated by Angiotensin II (of interest to those of you with CBS/BHMT problems,
Spironolactone is low in Sulfur). The ACE Del16 involves the insertion and
deletion of genetic material at a specific location (intron16) of the ACE gene,
coding for an up regulated, or over active Angiotensin Converting Enzyme. ACE
(+) individuals - I am ACE (+/+); yikes! - are at increased risk for
hypertension and cardiovascular disease. If you are ACE (+) and have problems
with BP or fluid control, we will have a low threshold for intervening
pharmacologically with ACEI and Spironolactone. Of interest, a large study
(HOPE) where a tissue specific ACEI (Ramipril, which like Quinapril enters the
vascular wall and preserves endothelial function) was administered to
individuals with diabetes and one other risk factor, demonstrated a reduction in
cardiovascular event and death rate over the ensuing five years. ACE (+)
individuals respond to statin drugs with larger reductions in cholesterol and
plaque burden than do ACE (-) individuals (who presumably have less need for
this form of intervention). Dr. Yasko recommends the use of Kidney Support RNA,
OraKidney, and OraAdrenal in kids with ACE problems. ACE may be associated with
increased anxiety; here she recommends use of the Stress and Anxiety Support RNA
product.
converting
enzyme inhibitors) target this enzyme, seeking to block generation of
Angiotensin II. The potassium and magnesium sparing diuretic Spironolactone
blocks the deleterious effects of Aldosterone, another mediator that is up
regulated by Angiotensin II (of interest to those of you with CBS/BHMT problems,
Spironolactone is low in Sulfur). The ACE Del16 involves the insertion and
deletion of genetic material at a specific location (intron16) of the ACE gene,
coding for an up regulated, or over active Angiotensin Converting Enzyme. ACE
(+) individuals - I am ACE (+/+); yikes! - are at increased risk for
hypertension and cardiovascular disease. If you are ACE (+) and have problems
with BP or fluid control, we will have a low threshold for intervening
pharmacologically with ACEI and Spironolactone. Of interest, a large study
(HOPE) where a tissue specific ACEI (Ramipril, which like Quinapril enters the
vascular wall and preserves endothelial function) was administered to
individuals with diabetes and one other risk factor, demonstrated a reduction in
cardiovascular event and death rate over the ensuing five years. ACE (+)
individuals respond to statin drugs with larger reductions in cholesterol and
plaque burden than do ACE (-) individuals (who presumably have less need for
this form of intervention). Dr. Yasko recommends the use of Kidney Support RNA,
OraKidney, and OraAdrenal in kids with ACE problems. ACE may be associated with
increased anxiety; here she recommends use of the Stress and Anxiety Support RNA
product.
Glutamate – GABA Imbalance Þ Excitotoxicity
Glutamate is the main excitatory neurotransmitter in the body. It is essential for learning and short and long-term memory. Glutamate is also the precursor to our primary inhibitory or calming neurotransmitter, GABA. GABA damps the propagation of sounds so that a distinction can be made between the onset of sound and a background noise. Many other physiologic processes require a balance between glutamate and GABA, which is usually easy to achieve as glutamate, glutamine, alpha-ketoglutarate, and GABA can be interconverted via the enzymes depicted above.
Genomic defects, viral illness, and heavy metals will compromise this balance, leading to excess glutamate, insufficient GABA, excitotoxicity, and eventual neuron loss. Viral infection (individuals with Methyl Cycle defects cannot defend well against viral infection) can lead to antibodies against the vitamin B6 dependent enzyme glutamate decarboxylase (GAD), blocking GABA production (this is felt to occur in the pancreas in kids with juvenile onset diabetes). Aluminum poisons this enzyme as well. Excessive alpha-ketoglutarate generated due to the CBS up regulation can be converted into glutamate, but in the presence of lead and aluminum, the glutamate so created cannot be converted into GABA, glutamine, or back to alpha-ketoglutarate. The result is glutamate-GABA imbalance, agitated behavior, and eventually nerve loss.
Low GABA leads to impaired speech, anxiety, aggressive behavior, poor socialization, poor eye contact, nystagmus, and constipation. Glutamate excess does the same and also wastes glutathione and increases levels of TNF-alpha, an inflammatory mediator that can produce heart cell dysfunction and gut inflammation.
We can restore glutamate-GABA balance by:
1. Addressing CBS up regulation/BHMT down regulations to
decrease alpha-ketoglutarate production.
2. Decreasing intake of food precursors of glutamate (see list below).
3. Supplementing with GABA
4. Copper inhibits conversion of glutamate to GABA by glutamate decarboxylase
so avoid copper excess, or better stated, an imbalance between copper and zinc.
5. Calcium is involved in glutamate toxicity, so supplement with magnesium to
keep calcium in check.
6. Remove heavy metals with a chelating agent. Of interest, toxicity due to mercury is aggravated by glutamate excess; mercury and glutamate synergize to damage nerve cells.
|
Sources of Excitotoxins – Short List* |
||||
|
Glutamate |
Glutamic acid, glutamine, MSG, peas, tomatoes, parmesan cheese |
|||
|
Aspartate |
Aspartame, Nutrasweet |
|||
|
Whey protein |
Soy protein |
Hydrolyzed anything |
Cysteine |
|
|
Malted barley |
Malt extract |
Natural flavoring(s) |
Guar gum |
|
|
Gelatin |
Carrgeenan |
Soy sauce |
Bouillon |
|
|
Vegetable gum |
Broth/Stock |
Yeast extract |
Autolyzed anything |
|
*Long list in the appendix
|
Treatment Options |
|
|
Pycnogenol and grape seen extract help balance Glutamate/GABA |
|
|
Taurine helps in this balance (but contains sulfur so avoid if CBS (+) |
|
|
Montief GABA |
|
|
ZEN |
Contains threanine, which has methyl groups; avoid if COMT (+) |
The Methyl Cycle abnormalities presented below are not as well understood (at least by myself):
MAO A: Monoamine Oxidase A
Monoamine Oxidase A breaks down serotonin, a neurotransmitter that is
generated from the dietary amino acid tryptophan, in a BH4 requiring reaction.
Many anti-depressant drugs, including the SSRIs (Serotonin Selective Reuptake
Inhibitors) work by blocking the breakdown of serotonin. Defects in serotonin
metabolism have been associated with mood and neurological disorders. How best
to address the MAO A R297R abnormality is not clear to me. As serotonin
metabolism is adversely affected, individuals with the R297R defect should avoid
large doses of high tryptophan foods (see appendix). High doses of St. John’s
Wort, often taken to address depression, could lead to mood swings as serotonin
levels fluctuate. Dr. Yasko recommends frequent dosing in small amounts of St.
John’s Wort, 5HTP (a tryptophan metabolite), and the Mood S RNA formula if
serotonin support is needed. If serotonin production is impaired on the basis
of BH4 deficiency secondary to a Methyl Cycle abnormality, as the abnormality
itself is addressed, BH4 levels should stabilize, hopefully normalizing
serotonin production.
ACAT 102: Acetyl Co-Enzyme A Acetyltransferase
ACAT is involved in cholesterol and energy metabolism, helping to
mediate the conversion of foodstuffs into biological energy. ACAT dysfunction
may lead to B12 deficiency. Right now, I do not understand ACAT well and am not
sure how important this is.
AHCY S-Adenosylhomocysteine Hydrolase
S-Adenosyl Methionine (SAMe), the key methyl donor generated from
methionine, is metabolized in to S-Adenosyl Methionine, and then on to
homocysteine by AHCY. Individuals (+) for both AHCY and CBS often have low
baseline urine sulfate levels, which then rise and fall in response to
treatment. Early on the levels rise, as the “bottle neck” abnormal AHCY enzyme
has been “limiting the supply” of homocysteine. Once the cycle starts to spin,
homocysteine is made available to CBS, and urine sulfate will rise. Later, in
response to a low animal protein/low sulfur diet, urine sulfate levels will
fall. Defects in AHCY are addressed by measures designed to improve overall
Methyl Cycle function, such as Methyl support RNA 1/8th dropper per
day.
VDR Fok
The VDR (Vitamin D Receptor) Fok defect affects blood sugar control and
pancreatic function. It does not affect dopamine metabolism. Dr. Yasko
recommends Vitamin K and generalized support of pancreatic function and sugar
regulation (low carbohydrate diet, supplementation with chromium, etc.) when the
VDR Fok abnormality is an issue.
Overview – Environmental toxicity (organic pollutants and heavy metals) is a grave threat to health – your health and that of your descendents. Lifestyle factors (which you can alter) interact with genomic “weak links” (which we can analyze and help you bypass) to determine at what age you will become ill (when the toxins will get to you). The most important thing that we can do (after getting you through an acute health care crisis) is to optimize your intracellular nutritional status, and then move Heaven and Earth to identify, and then remove, every toxic molecule from your body – to return your biochemistry to the pristine state that Evolution and/or Our Creator intended. A goal of Methyl Cycle analysis/treatment is to help you become a more efficient detoxifier. Toxicity testing and detoxification thus makes sense. These concepts are outlined below and are discussed in greater detail on heartfixer.com and in our presentations (DVDs and information sheets are available to you).
Diagnosis – Which toxins do you bear and why did you retain them?
1. Genomic Analysis: While we can and will detoxify you without knowledge of
your genomic status, an understanding of your inherited weak links will alter
(and improve) our approach.
Methyl Cycle Nutrigenomics: The Methyl Cycle is the backbone of your
biochemistry. Methyl Cycle defects prevent you from coping with environmental
toxins, viral and bacterial invaders, and compromise proper reading of your
genetic code. Chronic, difficult to explain disease states, neurodegenerative
conditions involving the young and premature “age related” conditions likely
reflect an interaction between environmental toxins and Methyl Cycle
predispositions. While we can’t change your DNA, if we know your weaknesses, we
can create nutritional “work arounds”, improving your ability to detoxify and
defend. Methyl Cycle testing is available (»
$550 via holisticheal.com and
»
$100 through 23andme.com). This information will alter the way I treat you.
Upon request, I can create a detailed analysis/treatment plan, based upon your
DNA findings, personal health and nutritional status, and toxin burden.
Detoxification Genomics: We vary in our ability to activate (Phase I) a
toxin, and then to combine it with a chaperone molecule (Phase II) that escorts
it out through the kidneys or GI tract. If I know your detox weak links then I
can support them with specific supplements/dietary interventions. Detox Genomic
testing is available through Genova Diagnostics (»
$500) or through 23andme.com (included in the $100 for your Methyl Cycle data).
2. Organic Pollutants: These are non-metallic, fat-soluble molecules that
bioaccumulate and compromise our physiology (and that of our offspring),
particularly with respect to weight gain, diabetes, and neurologic disease.
Agent Orange, phyllates, bisphenol A, pesticides, and petroleum products are a
few of the 100s of organic pollutants to which we (and our Mothers) have been
exposed to (yes, this stuff readily crosses the placenta). Fat, liver, and
nerve biopsies would give us the most complete measure of organic pollutant
burden but obviously are not practical. We can estimate your tissue pollutant
burden with:
A. The US BioTek organic pollutant screen looks at seven common organic
pollutants and compares your personal levels against that of the rest of the US
population. This $125 test is easily done at home (a dipstick is dipped in a
morning urine sample and then sent to the lab).
Its downside is that it weighted more towards recent exposure then to chronic
body burden.
B. The Genova Labs NutrEval gives us markers of Styrene and Petroleum product
exposure, along with a great deal of ancillary information regarding nutritional
and detox function. The NutrEval is covered by Medicare (not with Aetna/Humana
secondary); with commercial insurance the out-of-pocket co-pay is $170. This is
the best single test in Metabolic Medicine.
C. Metametrics provides more extensive organic pollutant testing, at a cost
between $ 250 and
$ 600. This is the best test available but perhaps not the best use of your
resources.
3. Heavy Metals: Metals enter our tissues, bind to proteins, and leave only
slowly - if at all (the half-life of mercury in the nervous system is 10-20
years). Metal exposure may vary, in relation to where you live and work, but as
innate detox is so slow, metals bioaccumulate. Tissue levels rise with age,
with a concomitant increase in your risk for metal-induced or metal-aggravated
disease states (conditions associated with inflammation or oxidative stress –
neurologic and cardiovascular). We need to estimate your body burden and then
remove these elements that can do nothing but harm. So how best to estimate the
level of metal accumulation within your internal organs?
A. Blood levels reflect recent exposure, and are of value in monitoring lead
exposure in kids, industrial exposure in adults, and in epidemiology studies.
However, blood metal levels bear little relation to body burden, and are not of
value in adult detoxification medicine.
B. Red cell metal levels tell us what your physiology has been exposed to over
the preceding three months. Red cell metals (and minerals) is included in the
NutrEval, or could be obtained for $ 136 from Drs. Data.
C. Provocative Challenge is the accepted best estimate of body burden. Here we
administer oral and IV metal binding agents, with metal quantitative in a
subsequent six hour urine collection. Your cost ($250) includes our fee, the
lab fee, and the IV and oral chelating agents utilized.
D. QuickSilver provides a blood, hair, and urine mercury assessment, and
estimates the percentage of your mercury burden that is organic vs. inorganic in
nature. Cost is $ 350.
Treatment
– How do we get this stuff out of you?
Methyl Cycle and Detoxification Genomic Abnormalities: Nutritional
supplementation and dietary avoidance measures are recommended, specific to your
individual inherited weak links.
Chelation Therapy: A generic term referring to the administration of
agents that bind to and then remove toxic metals (but not organic pollutants)
from your body.
1. Mg-EDTA: A series (20-30) of 3-hour IV infusions containing Mg-EDTA,
B-Complex and Vitamin C. Mg-EDTA was used in the NIH sponsored Trial to Assess
Chelation Therapy (TACT, which demonstrated an 18-38% reduction in 5-year
adverse event rate when chelation therapy was added to standard
pharmaceutical/interventional management in individuals with prior heart
attack). I have been treating my patients with Mg-EDTA for 20 years; we were
first amongst cardiology practices and third overall with respect to patient
participation in TACT). When Lead and Cadmium are the problem, EDTA is the
most effective chelator, and IV therapy is the most efficient approach. The
magnesium content is also helpful in BP management.
2. Ca-EDTA: Calcium-EDTA alone is infused over 10 minutes. With respect to
metal removal, both IV approaches are likely equally effective, but here you do
not receive IV nutritional support. We favor Mg-EDTA in individuals with
cardiovascular disease/hypertension and Ca-EDTA in younger patients (or if time
constraints preclude you receiving a three hour treatment).
3. Essential Daily Defense (EDD): EDD is a mixed oral chelator that is taken
concomitant to any IV chelation (blocks recycling of bound metals from the GI
tract back to the circulation).
4. DMPS: 25 years ago, our only toxin was Lead, and EDTA was all we needed.
Today we are being bombarded with “new and improved” toxins, particularly
Mercury. EDTA does not remove Mercury from your cells! We remove mercury with
“di-thiol” chelators: DMSA and DMPS. We can address Mercury toxicity with IV
DMPS, but the application of liposomal DMPS complexed with Glutathione to your
skin is easier for you and is more cost-effective. Compared to EDTA, DMPS binds
less avidly to Lead and is not an efficient Cadmium chelator.
5. DMSA: Available over-the-counter or by standard or compounded prescription,
DMSA will bind to and remove Mercury, Lead, and Cadmium, but DMSA is not as
powerful as EDTA or DMPS. DMSA is typically taken as 500 mg, 3 times a day,
over 3 consecutive days, once a month, or within a program of DMSA 500 mg near
bedtime, 10 nights on, 5 nights off.
6. Liposomal Phosphatidylcholine-EDTA (DetoxMax Plus): Liposomes of Phosphatidylcholine serve
as drug delivery vehicles for EDTA, dramatically enhancing its absorption
following oral administration. Lipophos EDTA serves as a slow and steady
approach to metal detoxification, of particular value to patients with vascular
insufficiency (please see our DVD presentation).
7. Med Five: Med Five is a patented enteric coated EDTA/phosphatidylcholine
tablet that we feel is better absorbed than standard oral EDTA preparations (see
www.medfive.com). I helped design Med Five and am a co-holder of its patent.
My personal patients can obtain Med Five at a discount (you receive a
password). The discount is a plus for you and resolves conflict of interest
concerns (otherwise I would not be able to talk to my own patients about a
health promoting approach that I helped create).
8. Battle Plan for Mercury: This protocol, which addresses heavy metal overload
with specific focus on Mercury, was developed by my mentor and good friend Dr.
Robert Battle. Dr. Battle Plan is typically run over 2-3 months and consist of:
A. Algas, 10 drops in 2 oz. of water (let it sit 1 minute before drinking) twice
a day – odd days,
B. NDF, 8 drops sublingual twice a day - even days (start at 1 drop and increase
as tolerated), &
C. Chlorella 5 twice a day, all days.
This protocol is typically well tolerated by individuals with CBS up
regulations, but if detox symptoms (fatigue, malaise, muscle aching) develop,
then the doses of Algas and NDF may be decreased. Dr. Battle often uses this
protocol to help clear Mercury before beginning Lead and Cadmium detoxification
with EDTA.
9. Metalloclear: This Metagenics product promotes metal and organic
pollutant detoxification. Nrf2, when translocated to the nucleus, codes for the
production of antioxidant and detoxification enzymes. Metalloclear promotes
nuclear translocation of Nrf2 and MTE (Metal Transcription Factor), which codes
for the generation of our endogenous metal binder Metallothionine.
Metallothione’s job in health is to store Zinc and Copper, but it will also
bind, and then transport to the liver for elimination, toxic metals such as
Lead, Cadmium, and Mercury. Monotherapy with MetalloClear involves three
tablets twice a day (with food) over 10 days, but we often use it as an
adjunctive or maintenance therapy at one tab twice a day.
10. Glutaclear: This Metagenics product provides N-Acetyl Cysteine, Selenium,
and Vitamin C, to increase Glutathione production, along with Broccoli extract,
to promote Nrf2 translocation. We typically recommend one tab twice a day.
11. Aura (Digital Homeopathy) Organ Detox Patches: Digital homeopathy is an
in-depth discussion (so we have DVDs, CDs, and handouts), but basically the
patches emit frequencies that permeate your meridian system and neutralize
toxins that you bear. The toxins will not be removed, but rather electrostatically neutralized (allowing us to remove them in a deliberate
fashion). We can’t prove that this method works, but I think it does, and it is
relatively inexpensive ($35 for a one month supply – typically worn over 2-3
months). This methodology can also be used to estimate your body burden of
toxins and screen for other health challenges.
12. Static Magnetic Field Chelation: Exposure to a static magnetic field
increases intracellular energy potential and increases the efficiency of any
metal chelation program that we might employ. This is the basis for MME and
magnetic sleep pad assisted chelation – a huge step forward! MME combined with
chelation is providing outcomes that aren’t supposed to occur – please review
the website to see what we are accomplishing. My personal patients receive a
discount when they purchase a negative field only sleep pad at magneticosleep.com.
13. Asyra Homeopathic Detoxification: Utilizing a physics similar to that
of the Aura Patches, our Asyra device imprints treatment frequencies, specific
to you, into a homeopathic carrier liquid – you take sublingual drops twice a
day. Asyra is repeated and new drops are generated every 2-3 months over 1-2
years. Again, we cannot prove this approach with an allopathic lab study, but
our observation is that our patients receive benefit from this approach.
14. Platinum Footbath: Your feet or hands are immersed in salt water, in to
which specific frequencies are applied. The water is ionized; the field enters
your body, and appears to break ionic bonds between toxins and your normal
molecules. The toxins are drawn out in to the water in a sort of “reverse
electroplating” or “forced sweating” effect. That toxins are being removed has
been verified by third party chemical evaluations (see Asyra.com). I’m not sure
whether metals can be removed by the footbath, but hydrocarbon toxins are, and
it seems to be particularly well suited to patients with gout. Footbath therapy
lends itself well to in-home use.
15. Glutathione Patch – Your body’s own production of Glutathione increases (and
blood levels rise) while you wear this drug free, non-transdermal skin patch
(see lifewave.com/chc).
16. Far Infrared Sauna (FIS): Sweat carries out with it toxic substances. We
sweat less as we age (aluminum containing anti-perspirants harm us here).
Regular sauna will sweat out toxins, but the extreme heat will not be tolerated
by many of you. FIS utilizes lower heat levels coupled with low level radiant
energy derived from ceramic plates to generate active sweating. FIS is
therapeutic in several cardiovascular conditions (FIS is covered under Medicare,
but we don’t offer this treatment - we can’t have people prancing around the
office in their bathing suits).
17. Frequency Specific Microcurrent (FSM): FSM applies frequencies (via skin
electrodes or a moistened towel) at 1/5000th the amplitude of the
TENS unit. While TENS therapy seeks to obliterate pain signals, with FSM we
seek to communicate with or entrain our physiology to carry out a desired
activity. FSM can be applied to many health challenges (see our information
sheet or www.frequencyspecific.com).
Costs – Your insurer will not cover the costs of any form of
detoxification therapy. They will describe it as “medically unnecessary” or
“experimental”. I will not write letters to request “pre-authorization” – this
is simply a waste of time and risks labeling you as a “troublemaker”.
Detoxification is a comprehensive and often long-term process, and it is not
inexpensive, but I think that you are worth it. Please consider what you spend
on a new car, or on a vacation, and then ask yourself what your health is
worth. If you do not wish, or cannot afford, to undergo detoxification, then we
can still help you - and we will help you - but our focus then (by necessity)
will be confined to nutritional intervention that you can afford and the
administration of insurance covered drugs and invasive treatments to deal with
the consequences of long-term toxicity. Why not prevent this? I personally
spend a lot of time and money on my personal health (supplements, detox, home
FSM, and lots of running shoes). I like the idea of vibrant health and a
vibrant mind, and I also realize that being sick ultimately will cost me more
than staying healthy. I also realize that “next day” and “fully covered”
surgical approaches to preventable health conditions may not be available to me
in later years (what is the wait time for bypass surgery or a knee replacement
in England or Canada)?
Politics – Leave this at the door. I am not interested in verbally sparing with other physicians who don’t know anything more about nutritional biochemistry and detoxification than I do about delivering babies or removing gall bladders. Do not expect me to compromise on science to meet the expectations of other doctors, insurance companies, or government agencies that just don’t understand (or wish to understand) the devastating consequences of organic pollutant and metal accumulation on our health and the health of our children and grandchildren.
Appendix I: Foods High in Tyrosine or Tryptophan
|
Foods High In Dopamine (or Amino Acid Precursor Tyrosine) |
|
|
Bananas, Red plums, Figs, Raisins |
Eggplant, Green Bean pods, Italian broad beans |
|
Salami, Sausage, Liver |
Commercial gravies and Soy sauce |
|
Salted dried fish (Herring, Cod) |
Canned meats, Aged game |
|
Canned meats, Aged game |
Homemade yeast breads |
|
Some alcoholic beverages (not all) |
Yeast concentrates, Marmite, soup cubes |
|
Aged Cheese (Blue, Boursalt, Brick,
Brie, Camembert, Cheddar, Colby, Emmental, Gouda, |
|
|
Foods High In Serotonin (or Amino Acid Precursor Tryptophan) |
|
|
Turkey, Chicken, Chicken Liver, Tofu |
Almonds, Peanuts, Soy Nuts |
|
Milk, Yoghurt, Cottage cheese |
Spirulina (seaweed), Brewer’s yeast |
|
Watermelon Seeds |
|
Appendix II: Foods High in
Sulfur
(but please review Sulfites and Chronic Disease, by Rick Williams
(available at the office or you can go to www.readingtarget.com/nosulfites)
Dietary Sulfur Issues
Sulfur is necessary for many metabolic functions, but sulfur deficiency is rarely an issue, as most foods contain sulfur or sulfur containing compounds. Excess sulfur can be a problem for those with CBS, BHMT, and SUOX mutations – here one needs to avoid foods and supplements high in sulfur (sulfites and sulfates).
|
Supplements High In Sulfur |
|||
|
Taurine |
Cysteine |
Methionine |
Glutathione |
|
Glucosamine Sulfate |
Chondroitin Sulfate and MSM |
||
|
Epsom Salts |
Magnesium Sulfate Cream |
||
|
Canned meats, Aged game |
Homemade yeast breads |
||
|
DMSA and DMPS (Metal Chelators) |
Milk thistle, Beyond C, and Heparin |
||
|
Foods High In Sulfur |
|||
|
Vegetables: |
|
|
|
|
Garlic, Onion Family |
Kale |
Collards |
Pickles |
|
Cabbage |
Brussel Sprouts |
Kohlrabi |
Broccoli |
|
Cauliflower |
Bok Choy |
Mizuna |
Broccoli Rabe |
|
Chinese Cabbage |
Napa Cabbage |
Turnip / Rutabaga |
Canola / Rape Seeds; Greens |
|
Mustard Seeds |
Tatsoi |
Radish |
Daikon |
|
Horseradish |
Japanese Horseradish |
Arugula |
Watercress |
|
Peas |
Spinach |
|
|
|
Fruits: |
|
|
|
|
Raspberry |
Cranberry |
Currents |
All Dried Fruit |
|
Others: |
|
|
|
|
Vinegar (especially if prepared from wine) |
|
||
|
Alcohol Beverages (especially wine; not vodka - beer is less of an issue, especially German beer) |
|||
|
Soft Drinks |
Animal Products |
Dairy |
Eggs |
|
Brazil Nuts |
Peanuts |
Soy |
|
All packaged and commercially prepared foods contain food additives, many of which contain sulfur; often this is not on the label. Organic foods are preferable here. Do not begin taking horsetail grass, spirulina, dandelion leaf, or parsley, as they contain low levels of sulfur. If they are already part of your protocol, you may continue taking them. Eliminate them only if having trouble turning your strips pink. Recognize that methionine and SAMe do contain sulfur, as do the sulfur containing amino acids taurine and cysteine. After strict sulfur elimination for 3 to 4 months you will have eliminated the deep stores of sulfur in your body. Thereafter, you can begin adding very small amounts of sulfur and ammonia producing products back into your diet, while watching your strips to be sure they stay pink.
“What Can I Eat?”
Low Sulfur Foods:
¨ Quinoa hot & cold in salads or with fruit
¨ Brown rice, non-gluten grains
¨ Fruit (except those on the high sulfur list)
¨ Vegetables (except those on the high sulfur list)
¨ Small amount of beans
o Lentils
o White Beans
¨ Small amount of nuts (except those on the high sulfur list)
o Macadamia
o Pine
o Cashew
o Pistachio
o Walnuts
o Almonds
o Pumpkin
o Sunflower seeds
o Chestnuts
¨ Make milk from nuts: soak almonds overnight.
¨ Bamboo Shoots
¨ Corn
¨ Mung Bean Sprouts
¨ Boiling removes much of the sulfur from foodstuffs (make sure you discard the water)
Meals:
¨ Alkaline vegetable soup:
Add cut carrots, green beans, zucchini squash, and celery to alkaline water.
Simmer one hour; flavor with salt as needed.
¨ Vegetables with olive oil and salt or other flavorings – add quinoa to make a meal
¨ Plain millet and Kamut cereal puffs with nut or rice milk and fruit
¨ Plain Mochi puffs, stuffed with apple, berry, or spicy sauce
¨ Sauté squash and other vegetables in olive oil and top with non gluten grain
¨ Healthy Fries:
o Cut up sweet and/or white potatoes in strips and coat with oil and seasoning. Lay flat on baking sheet and bake until crispy.
¨ Salads without high sulfur veggies and dressing.
¨ Apple or berry sauce mixed with flax seed
¨ Nut-Milk Shake:
Take frozen fruit chunks, stevia, fiber such as flax and blend with rice or nut milk until smooth
¨ Cut vegetables, mix with olive oil and seasonings and bake
¨ Brown rice tortillas chips:
Coat pan with olive oil. Cut up brown rice tortillas (found at Trader Joe’s) place on baking sheet. Season as desired, and bake until crispy.
¨ Vegan burger:
Combine cooked sweet potato or yams, quinoa, chopped vegetables, salt or other seasonings. Add enough non gluten flour (chickpea, rice), and form into patties. Brown in olive oil.
¨ Mashed Squash:
Take acorn, butternut, or other hard squash and steam. Mash with xylitol and cinnamon, nutmeg, or ginger.
¨ Squash Fries:
Take acorn, butternut, or other hard squash and cut in half. Cut into thin slices and bake flat until crispy.
¨ White bean or lentil soups with rice crackers.
¨ Cold quinoa with cut vegetables and Italian dressing.
¨ Boil vegetables like potatoes and dress with olive oil and seasoning.
Appendix III: Foods High in Excitotoxins
|
Sources of Excitotoxins |
|||
|
Glutamate |
Glutamic acid, glutamine, and MSG. High levels are found in foods such as peas, tomatoes, parmesan cheese, milk, mushrooms, fish, and many vegetables |
||
|
Aspartate |
Aspartame, NutraSweet |
||
|
Other “Names” for Excitotoxins |
|||
|
Monosodium Glutamate |
Glutamate |
Natural Flavor(s) |
|
|
Maltodextrin |
Carrageenan |
Gelatin |
Spice(s) |
|
Seasoning(s) |
Seasoned Salt |
Dough Conditioner(s) Isolate |
|
|
Autolyzed Yeast |
Autolyzed Yeast Extract |
Autolyzed Anything |
Broth |
|
Stock |
Soup Base |
Chicken/Pork/Beef “Flavoring” |
|
|
Hydrolyzed Vegetable Protein (HPV) |
Hydrolyzed Plant Protein |
||
|
Hydrolyzed Oat Flour |
Hydrolyzed Anything |
Yeast Extract |
|
|
Sodium Caseinate |
Calcium Caseinate |
Caseinate |
Disodium Guanyiate |
|
Disodium Inosinate |
Disodium Caseinate |
Hydrolyzed Protein |
Chicken/Pork/Beef “Base” |
|
Bouillon |
Vegetable Gum |
Plant Protein Extract |
Smoke Flavoring(s) |
|
Malted Barley Flour |
Malt Extract |
Malt Flavoring(s) |
Malted Barley |
|
Malted Anything |
Textured Protein |
Guar Gum |
Soy Extract |
|
Soy Protein |
Soy Protein Concentrate |
Soy Sauce |
Whey Protein |
|
Whey Protein Isolate |
Whey Protein Concentrate |
L-Cysteine |
|
|
Ajinomoto |
Kombu Extract |
Natural Flavoring(s) |
Barley Malt |
|
Foods with MSG (Monosodium Glutamate) |
|||
|
Hydrolyzed Protein |
Hydrolyzed Oat Flour |
Sodium Caseinate / Calcium Caseinate |
|
|
Gelatin |
Glutamic Acid |
Monosodium Glutamate |
|
|
Autolyzed Yeast or Yeast Extract |
|
|
|
|
Possible Sources of MSG |
|||
|
Textured Protein |
Carrageenan Or Vegetable Gum |
Seasonings Or Spices |
Flavorings Or Natural Flavorings |
|
Chicken, Beef, Pork, Smoke Flavorings |
Bouillon, Broth, Or Stock |
Barley Malt, Malt Extract, Malt Flavoring |
Whey Protein, Whey Protein Isolate, Or Concentrate |
|
|
|||
|
|
|||
|
|
|||
|
Other Sources of MSG |
|||
|
Food From Fast-Food Chains |
OTC Medications |
Chicken Pox Vaccine |
|
|
NutraSweet |
Binders and Fillers in Supplements |
Prescription Medications |
|
|
Foods with Glutamates |
|||
|
Doritos |
Pringles |
KFC Fried Chicken |
Boar’s Head Cold Cuts/Hot Dogs |
|
Progresso Soups |
Lipton Soups/Sauces |
Gravy Master |
Planter’s Salted Peanuts |
|
Sausages / Processed Meats / Cold Cuts |
Processed Cheese Spread |
Molasses |
Supermarket Turkey And Chicken (Injected) |
|
Restaurant Gravy |
Ramen Noodles |
Bouillon |
Instant Soup Mixes / Stocks |
|
Salad Dressings / Croutons |
Salty, Powdered Dry Food Mixes |
Flavored Potato Chips |
Restaurants Soups Made From Soup Base |
|
Gelatin |
Soy Sauce |
Worcestershire Sauce |
Kombu Extract |
|
Dry Milk Or Whey Powder |
Dough Conditioners |
Body Builder Protein Mixes |
Parmesan Cheese |
|
Fresh Produce Sprayed With Auxigro In The Field |
Some Spices |
Skim, 1%, 2%, Non-Fat, Or Dry Milk |
Whipped Cream Topping Substitutes |
|
Non-Dairy Creamers |
Chocolates / Candy Bars |
Low-Fat / Diet Foods |
Cereals |
|
Baked Goods From Bakeries |
Frostings And Fillings |
Catsup |
Mayonnaise |
|
Chili Sauce |
Mustards |
Pickles |
Bottled Spaghetti Sauce |
|
Citric Acid Made From Processed Corn |
Canned And Smoked Tuna, Oysters, Clams |
Barbeque Sauce |
Canned, Frozen, Or Dry Entrees And Potpies |
|
Fresh And Frozen Pizza |
Flavored Teas, Sodas |
Seasoned Anything |
Some Bagged Salads And Vegetables |
|
Tomato Sauce / Stewed Tomatoes |
Egg Substitute |
Flour |
Canned Refried Beans |
|
Tofu And Other Fermented Soy Products |
Table Salts |
Anything With Corn Syrup Added |
Anything With Milk Solids |
|
Anything Fermented |
Anything Vitamin Enriched |
Anything Protein Fortified |
Anything Enzyme Modified |
|
Anything Ultra-Pasteurized |
Carmel Flavoring/Coloring |
Pectin |
Cornstarch |
|
Flowing Agents |
Xanthan Gum / Other “Gums” |
L-Cysteine |
|
Appendix IV: Elevated Urine Sulfate - What Do You Do Next?
Elevated Urine Sulfate – Above 1600 mg/liter
You are receiving this communication because a spot urine sample returned with an elevated sulfate level. As you are by now aware, we are actively involved in Methyl Cycle Genomic testing, looking for the underlying “common denominator” causes of the otherwise difficult to explain and address disease states with which many of our patients present. The vast majority of chronically ill or unexplained ill individuals who we have tested have demonstrated abnormalities in the Trans-Sulfuration pathway of Homocysteine metabolism. Dietary change, medication adjustment, and specific nutritional support, all tailored to the individual’s genotype, can lead to a major change in the health of these individuals.
Methyl Cycle testing is expensive: $1,150 for the testing, analysis, and recommendations. Obviously it doesn’t make sense to test every patient who we see, but on the other hand it doesn’t make sense to keep doing the same ineffective thing over and over because we really do not know why a chronically sick person is chronically sick.
There are clinical “tip offs” to a Trans-Sulfuration pathway defect, the most important of which is an elevated urine sulfate level (the CBS up regulation and/or BHMT down regulations force Homocysteine down the Trans-Sulfuration pathway, generating excessive sulfite/sulfate). Methyl Cycle Genomic testing costs $1,150, while the urine sulfate test costs $10 - so we carried out the urine sulfate test in you and it returned above 1,600 mg/liter.
So what exactly does this mean? What should you do know? Is the study 100% diagnostic? Right now, we do not have absolute answers to these questions; nor does anyone else. However, we are on to something very important here and it likely affects you.
The questions that we have regarding the link between urine sulfate and the
presence/absence of a specific genomic defect are:
A. Is an elevated urine sulfate diagnostic of a Methyl Cycle defect?
B. Are there false positives (high sulfate with normal genes) and false
negatives (low sulfate and abnormal genes)?
C. Is there a quantitative relationship between the sulfate level and the
severity of the genomic impairment?
D. Will the sulfate level vary day to day and with time of day or meals?
We are comparing the urine sulfate levels against the genomic findings in all patients who are undergoing genomic testing. My initial impression is that individuals with markedly elevated urine sulfate levels all have CBS and/or BHMT abnormalities. We have seen a few false negatives (CBS/BHMT abnormality present but urine sulfate only in the 400 mg/liter range); these individuals have “upstream” abnormalities that limited Homocysteine production, giving CBS/BHMT less homocysteine to force down the Trans-Sulfuration pathway, or a “downstream” defect in SUOX (Sulfite Oxidase), such that sulfate could not be generated from sulfite (the entity actually generated by CBS), and/or they were already on a Vegan type diet. So far we have not identified any false positive patients, and when patients with known CBS/BHMT abnormalities switch to a low sulfur, low animal protein diet, their urine sulfate levels do fall. Still, there could be causes for a false positive study. Many drugs and nutritional supplements are loaded with sulfite/sulfate (typically not a problem for individuals who do not harbor Trans-Sulfuration defects). It is not inconceivable that if you take these drugs or supplements that your urine sulfate will be elevated regardless of your genomic status.
So what should you do with this information? If money is not a concern, then undergo Methyl Cycle testing. Knowledge as to what is wrong with you (or what could go wrong with you in the future) can only help us optimize your health. If money is an issue but you wish to take some positive steps, you could change your diet “as if” you have a CBS/BHMT abnormality, and this is a better diet than the one most of us are currently following. We could also, in a step-by-step fashion, adjust your drugs and nutritionals while watching your urine sulfate level. The supplements we use in CBS/BHMT individuals are all benign. Please review the attached instruction sheet. You can learn more at our monthly Methyl Cycle support group meetings (third Monday of every month at the Secor Clarion - $5 admission) and by studying the information discussed above in this section of the website. You can also review Dr. Yasko’s website holistichealth.com, keeping in mind that her focus is on Autism, while ours is on adults with chronic or unexplained illnesses. You could also wait. As we gain more experience in this area, our diagnostic and treatment methods will evolve and improve – it‘s always been this way.
Again, we will have more definitive information in the future, but this is too important a concept to just “sit on”; thus the urine sulfate screening, this letter, and our invitation to you to learn more.
Appendix V: General Recommendations Based Upon the Sulfate Value
Approach to Patients with Presumed Trans-Sulfuration Pathway Abnormalities
Methyl Cycle Genomic analysis is demonstrating Trans-Sulfuration (CBS up regulation or BHMT down regulation) abnormalities in 90% of our patients with unexplained disease states who undergo testing. Dietary change and nutritional supplementation, designed to fit the genotype of the patient, is turning around the lives of some previously quite ill people. The “tip offs” to a Trans-Sulfuration Methyl Cycle defect are sulfite sensitivity (and to a lesser extent asthma and easy bruising), a low or low normal homocysteine level, and an elevated urine sulfate level – but so far sick people who are not getting better all seem to have this problem! Methyl Cycle testing is expensive - $1,150. Some individuals may choose to omit Methyl Cycle testing and proceed directly to treatment, as if they have this genomic defect. Others may wish to take action while waiting the two months for the lab results to return. As there is nothing inherently dangerous about our approach to CBS/BHMT dysregulation, this approach is medically reasonable. The following general recommendations make sense for individuals who may harbor a Trans-Sulfuration pathway abnormality and who do not wish to undergo Methyl Cycle testing or who do not wish to wait until their lab results return.
Overview
We assume that you are +/- or +/+ for one of the CBS up regulations and +/+ or +/- for BHMT 1-8, which act like CBS up regulations. Homocysteine (as well as its methyl cycle precursors) is being drawn down the transulfuration pathway, in this process generating too much sulfite and sulfate (which stimulate the stress/cortisol “fight or flight” response), too much alpha-ketoglutarate (which leads to excitotoxin activation), and too much ammonia, which depletes BH4 (leading to insufficient dopamine and serotonin production, and a lack of nitric oxide).
To
address CBS up regulation/BHMT down regulation we typically recommend:
1. No animal protein diet (anything with eyes) and avoid sulfur rich vegetables,
sulfur containing supplements, and sulfur containing drugs (see CBS and
Appendix II: Foods High in Sulfur and/or read Sulfites and Chronic Disease
by Rick Williams, available at the office or at www.readingtarget.com/nosulfites/.
2. Monitor urine sulfate every 4-7 days. Low levels (400 or 400-800 mg/liter)
will allow an increase in methyl cycle supplementation and later the addition of
BH4 and/or a liberalization of your diet.
3. To neutralize ammonia, use Ammonia Support RNA, a charcoal supplement at
bedtime (away from other supplements; magnesium citrate may be used as needed to
keep the GI tract moving as charcoal may lead to constipation), and Yucca.
These supplements can be tapered down as ammonia levels fall.
4. Molybdenum to help SUOX break down sulfite into less toxic sulfate.
Homogenized dairy products contain xanthine oxidase, which uses up molybdenum,
and are best avoided or minimized. Vitamin E succinate, Boron, and B12 are felt
to stimulate SUOX activity (SUOX is “overworked” by the sulfite load presented
to it by CBS/BHMT - SUOX co-factors become depleted, thus the need for
supplementation).
5. Avoid excitotoxins (see list on heartfixer.com) and supplement with GABA
twice a day.
6. Minimize B6, which stimulates CBS; P-5-P will be less of an issue.
7. Co-Q, Carnitine, Idebenone, and NADH will help increase energy production;
supplementation will be helpful but probably not critical.
8. After your sulfur and ammonia pools have been depleted down towards normal we
can be more liberal with other methyl cycle supplements, and/or add in BH4. We
do not wish to aggressively correct other methyl cycle defects until we have the
CBS issue under control – otherwise the intermediates that we do supplement or
generate will fall down the “CBS drain” into ammonia, sulfate, and
alpha-ketoglutarate. Thus the first priority is to decrease blood and urine
ammonia levels (easy to achieve with diet and supplementation) and urine sulfate
levels (this will take time – likely several months).
Plan of action for CBS/BHMT
1. Begin the diet discussed above and the supplements described below..
2. Check the sulfur (sulfite) content of your medications and supplements, and
we will try to phase out anything high is sulfur.
3. Monitor urine sulfate every 4-7 days (and please chart the levels) – this
will be our primary measuring stick – our goal is 400 mg/liter (one
yellow and three pink).
4. To neutralize ammonia, use Ammonia Support RNA ½ dropper with meals and with
methyl cycle supplements, along with a charcoal supplement at bedtime (away from
other supplements; magnesium citrate may be used as needed to keep the GI tract
moving as charcoal may lead to constipation). Yucca, beginning at ½ capsule,
twice a day, (or sprinkled on food containing protein), may help with ammonia
detoxification.
5. Regarding nutritional support, your current multi likely contains B6. A
better program involves the Yasko NHF multi, two twice a day along with Trace
Minerals Complex at 4 drops/day. Begin Molybdenum 3 drops twice a day, Boron 3
mg/day, and hydroxy-B12 2000 mcg daily to stimulate SUOX (the enzyme that
converts sulfite in to less toxic sulfate). These are the key nutritional
interventions.
6. Co-Enzyme Q10 100 mg/day, Carnitine 500 mg twice a day, and NADH one per day
are ideal but not critical.
7. Add GABA 500 mg once a day to blunt excitotoxicity; if you feel that GABA is
helping a lot then you can increase the dose; if it is not doing anything for
you then it can be discontinued.
8. If not already done, baseline Vitamin D, homocysteine, and ammonia levels
will be helpful (and will be considered at your next office visit).
9. In eight weeks (ideal but obviously not mandatory) we can carry out a 24 hour
urine for ammonia and amino acids and a separate 24 hour urine for nutritional
and toxic metals, and use the results to refine your supplementation program. If
a 24 hour urine collection is not possible than we could use a first AM void
urine for the ammonia/amino acid levels and a red cell mineral study.
10. Lipophos Forte 900 mg/day will stimulate BHMT, thus drawing homocysteine
away from the CBS “drain”. Lipophos EDTA, ½ bottle twice a week, will also
remove heavy metals, the clearance of which appears to be reduced in individuals
with Methyl Cycle abnormalities.
Appendix VI: Methyl Cycle Recipes
Veggie Organic Soup
2 T. Olive Oil
3 Stalks Organic Celery (sliced ¼”)
6-8 oz small Organic Carrots
3 T. Fresh Basil
2 T. Fresh Oregano
2 small Zucchini (green and yellow) sliced ¼”
1 T. Celtic Sea Salt
1 T .Fresh Ground Pepper
Sauté about 15 min
Add 2 L. Alkaline Water (about 2 quarts) then add
2 Fresh Tomatoes (peeled and chopped) to peel/score add to boiling water 15-30
sec.
watch for peel to come off then add to ice bath or 1 can 14.5 oz Organic
diced Tomatoes
2 15oz cans white beans rinsed and drained
12 oz fresh long cut Green Beans
Bring to Boil 20 min/ add more sea salt and pepper to taste
The last 6-7 min add 1 cup Quinoa Pasta Veggie Curls
In a separate pot boil 6-8 Gold Potatoes until tender
Add half of potatoes to soup/ the other half mash until creamy (this will give
the soup a creamy texture)
Do Your Best to buy All Organic—Enjoy!
Created by Cheryl Church
Orange Spaghetti Sauce
2 T. Olive Oil
3 Stalks Celery/diced
1 Orange Bell Pepper/diced
1 Med Carrot/diced
Sauté until tender, and then add
1 T. Oregano
1 T. Celtic Sea Salt
1 T. Black Pepper
3- 14.5 oz can Dice Tomatoes
Sprinkle small amount of Sugar to cut acid if desired
Bring to boil and simmer about 20-30 minutes
Cook 8 oz box of Quinoa Pasta Spaghetti Noodles
Sprinkle with chopped fresh Basil
Serve with long cut Green Beans or Zucchini chopped and sauté in Olive Oil
Makes about 5 cups sauce
Created by Cheryl Church
Quinoa and Yam Salad
1 cup Quinoa
2 cups water
3 cups yams/ chopped
2 T. olive oil
1 medium red bell pepper/chopped
1 tsp cumin
¼ cup fresh cilantro/chopped
2 T. Fresh lemon juice
1 T. Brown Rice Vinegar
1 T. Real Maple Syrup
In a medium saucepan, stir together the quinoa and water.
Bring to a boil, cover and reduce heat to medium low. Simmer for 15 minutes or
until cooked. Fluff with a fork and set aside to cool. In a large frying pan on
medium heat, sauté the yams until they are tender but firm to the bite. Add the
peppers and cumin and sauté for an additional 2 minutes. Set aside until cool.
In a large bowl, combine the quinoa, yams, cilantro, lemon juice, vinegar and
maple syrup. Mix well and cool in refrigerator.
Serve chilled.
Makes 6 servings
Recipe altered from The Garden of Vegan by Tanya Barnard & Sarah Kramer
Breakfast Ideas
#1 Quinoa Flakes/ Hot Cereal
Any kind of Fruit ( blueberries, peaches etc)
1-2 tea, cinnamon
1-2 tea real maple syrup
# 2 Brown Rice Crisps
Fruit (blueberries)
Rice Milk
#3 Roasted Potatoes with beets ,zucchini, peppers whatever veggie you like. Drizzle with Olive Oil. Bake at 350 degree oven for 20-25 minutes Season to taste.
Snacks
#1 Almond Butter with Rice Cakes and Bananas
#2 Almond Butter with Celery
#3 Bean Dip
1 can 15 oz Great Northern Organic White Beans
1 Fresh Lemon/ juiced
1 tsp. Celtic Sea Salt
Blend in food processor until smooth
Sprinkle with chopped fresh parsley
Serve with Rice Chips or Sweet potato and Beet Chips
#4Avocado Dip
1 medium size avocado/mashed with potato masher
1 chopped medium tomato
1 fresh squeezed lemon
1 T. coarse ground black pepper
Mix well and serve with Rice Chips
#5 Smoothies
1 large Banana
4-5 large Frozen Strawberries
1 cup Rice Milk
Blend until smooth /Freezes well
Spiced Squash Soup
Bake @ 350 degree oven
1 large Butternut Squash, brush with olive oil and bake until golden brown
about 1 hour
3 stalks of celery (chopped)
2 small sweet potatoes (peeled and chopped)
1 large apple (peeled and chopped)
1 T. olive oil
Sauté 4 above items until a little brown then add 3 cups alkaline water or filtered water, 1 tsp Celtic sea salt, 1 tsp. fresh cracked pepper, 1 bay leaf, ¼ tsp cinnamon, ¼ tsp cumin, ¼ tsp thyme, 1/8 tsp red pepper (cayenne) and a dash of nutmeg. Simmer for 15 minutes. Add all to blender and mix until smooth. Sprinkle with fresh basil and small amount of Parmesan Reggiano.
Makes about 6-7 cups
To add protein serve over quinoa pasta.
Created by Cheryl Church
Corn and Potato Chowder
2-3 T. olive oil
2 ½ cups chopped organic celery
4 cups organic corn (from can or cut from cob)
Sauté until celery is a little tender.
Add 4 cups chopped red skin potatoes, 1 T. Celtic Sea Salt, 1 T. Fresh cracked
pepper, if you like pepper this soup tastes great with lots of black pepper, 1
T. Celery Blend a product made by Celtic Sea Salt Selina Naturally.
Cover with alkaline water or filtered water. Bring to boil and simmer until
potatoes are tender about 15-20 minutes.
In separate pot boil 4 cups chopped red skins potatoes to mash and add to soup for creamy texture.
To add protein serve over cooked quinoa.
Created by Cheryl Church
Nutrtigenomic Supplements and Supplies
|
Nutrigenomic Supplements and Supplies (* are available at office) |
|||
|
Holistic Health (Dr. Yasko) |
www.holisticheal.com |
||
|
Emerson Ecologics |
www.emersonecologics.com(access code: chctol & zip: 43606) |
||
|
Life Extension Foundation |
ww.lef.org |
||
|
Order Code |
Supplement |
Source |
Comments |
|
Amazon.com |
Sulfate Test |
QFix |
$33 for a package of 100 sulfate test strips |
|
SKU:540 |
See RNA |
HH |
Ammonia support (neutralizes ammonia)* |
|
SKU:560 |
Products |
HH |
Methylation support (general methyl cycle support)* |
|
LORNA |
Orn/Aspartate |
EE |
Ornithine/Aspartate 3 gm/tsp – 100 doses for $66.97 |
|
SKU:02041 |
Yucca* |
HH |
600 mg – 60 for $17.46 |
|
SKU:01129 |
Charcoal* |
HH |
100 260 mg capsules for $9.99 |
|
Nutramedix |
Sparga* |
|
1.0 oz. bottle for $18 (nuramedix.ec) |
|
SKU:30054 |
Multi |
HH |
Dr. Yasko’s multi – 120 for $32 |
|
MOLY5 |
Molybdenum |
EE |
500 mcg tabs, 60 for $11.60 |
|
SKU:01092 |
Hydroxy-B12* |
HH |
Perque 2000 mcg hydroxy-B12, $28.95 |
|
COM28 |
CMC* |
EE |
Complete Mineral Complex - 90 capsules for $18 |
|
BOR04 |
Boron |
EE |
3 mg – 100 for $6.50 |
|
ECA21 |
Vit E Succinate |
EE |
400 IU – 100 for $$32.50 |
|
GABA 7 |
Montiff GABA* |
EE |
500 mg Montiff GABA, 100 for $21 |
|
SKU:01023 |
Zen* |
HH |
275 mg GABA and 100 mg Theanine – 60 for $21 |
|
01904 |
NAD+ |
LEF |
100 mg tabs, 30 for $34 |
|
CAR48 |
Carnitine* |
EE |
Carnitine 500 mg – 60 for $39.90 |
|
Office |
Q-Best* |
Thorne |
Co-Enzyme Q, 50 mg – 60 for $36 |
|
Office |
Ribose* |
Valen |
5 gm/dose; 50 doses for $56 |
|
00537 |
Methyl-B12* |
LEF |
5 mg chewable tablet - 60 for $32 |
|
Office |
DetoxMax* |
BI |
Phosphatidyl Choline with EDTA – 1 bottle for $30 |
|
Office |
Phoschol* |
ARG |
Phosphatidyl Choline 900 mg – 100 for $74 |
|
SKU:01043 |
PS* |
HH |
500 mg phosphatidyl serine – 60 for $39.90 |
|
CREAT |
Creatine |
EE |
Creatine 5 gm/tsp. – 20 doses for $24.50 |
|
L19 |
Lithium |
EE |
5 mg Lithium Orotate 90 caps for $19 |
|
Office |
Iodoral* |
|
12.5 mg – 90 for $27 |
|
TMG |
TMG |
EE |
750 mg TMG – 100 caps for $15.60 |
|
SKU:01088 |
Quercetin Plus* |
HH |
Quercetin 500 mg with Bioflavonoids – 50 for $14.05 |
|
00453 |
SAMe* |
LEF |
200 mg SAMe – 50 for $33.75 |
|
SKU:02017 |
Folapro* |
HH |
5-methyl folate 800 mcg, 60 for $19 |
|
FOL17 |
Folinic Acid |
EE |
800 mcg/tablet - 60 for $11 |
|
|
Methyl Folate |
Drug |
Metanx: 2.8 mg methyl folate, 25 mg P5P, 2 mg methyl-B12 |
|
|
BH4* |
|
BH4, 2.5 mg, 60 for $70 |
|
Office |
Glutathione* |
|
15 for $90 (each should last x 7 days) - lifewave.com/chc |
|
Office |
Book* |
|
Sulfates and Chronic Disease - $60 |
Office prices may be different – to include shipping and handling (5/25/15)
How to Order Supplements from Websites
Ordering from Holistic Health website:
· Go to www.holisticheal.com
· Click on Advance search
· Scroll down to box that states “Search for product”
· Click on Advance search option
· You will see: search category:
sku:
price:
· Enter sku # from list for the product you are looking for
· Click on search
· Under Quantity enter how many you want to order
· Click on add all items to cart
· Screen will show items in cart
· Click on Advance search and follow same protocol until all items are in cart
· Then click “check out”
· Review order and select delivery option
· If everything is ok then where you see update click “GO”
· Enter your delivery information and submit
· Follow directions for payment
Ordering from Emerson Ecologics
· Log onto www.emersonecologics.com
· On left side of screen click on “Product search”
· Enter code from list in box “By Product Code”
· Do not use any spaces with letters or numbers
· Check selection box
· Click add to shopping cart
· Then click add more product
· Follow same protocol for other items
· When all items are selected proceed to check out
· Follow directions to “Register Now”
· Click “I am a patient”
· Click continue
· Enter all info requested
· Click continue and follow directions for payment
Ordering from Life Extension Foundation
· Log onto www.lef.org
· On right side of screen enter product code in Search Catalog Number
· Then click add to cart
Methyl Cycle Genomic Testing and Treatment - What you Can and Cannot Expect from Us
We got involved in Methyl Cycle testing not because we had to, and not because we don’t have anything else to do. No - we got involved in Methyl Cycle testing for the usual reason, to
Help Patients Who We (and Nobody Else in the Area) Could Previously Help
This is why we were the 2nd practice in Ohio to get involved in EECP 12 years ago. This is why we brought MME to town 4 years ago, and why we continue to bring innovative and low risk diagnostic and therapeutic modalities to NW Ohio. We do this because our current best methods are not good enough; there are always patients who we cannot help so we are always looking for better methods (and these days the developers of better methods are bringing them to us).
New treatments, especially new treatments not available elsewhere in the area, always generate a lot of questions. We’d like to answer all of your questions, on an individual basis, and do so in a timely fashion, but in reality we can’t. We realize this and we need you to realize this as well. Staff members cannot answer questions regarding the biochemical genetics of specific Methyl Cycle pathways, just as they can’t explain the biophysics that allow the Glutathione patch to work or the bioengineering that allows the MME machine to regenerate damaged cells.
Dr. Roberts can answer these questions (well, most of them), but he cannot answer them for you, on an individual basis, outside of your office visits – it’s just not logistically possible. If you cannot accept this then please undergo Methyl Cycle Genomic testing elsewhere. Your $1,125 fee covers the cost of the laboratory Methyl Cycle testing, Dr. Yasko’s report, and Dr. Roberts’ analysis and recommendations, which integrates the Methyl Cycle findings into your past and current medical status. It takes Dr. Roberts considerable time to write what will be a 4-5 page report – but you are paying for this – and you are getting value for your money.
We have added to our program various means by which you can learn more, ranging from our monthly Methyl Cycle support group meetings to individual sessions with Krista McCarthy Mignin MS. Take advantage of these resources.
Please do not call the office with open ended questions or requests such as “I want someone to explain this to me” or “I want Dr. Roberts to call me”. We can’t do this. All of you know how hard I work. I am so busy with our current programs that I had to give up all past hospital activities except for doing heart catheterizations every other Thursday. I am not going to call you up (and you may not answer your phone at night or on weekends) to answer non-emergency questions, the answer to which 75% of the time will be in my written report.
Please do not call with questions like “what can I eat”, or “is a certain food OK”? We do not have ready answers to these questions. We do put a lot of information regarding diet in to our Methyl Cycle reports. We do give you resources where you can learn more, but please remember, we are not dietitians nor are we nutritional counselors (but Krista McCarthy Mignin is). Also, please avoid expressing anger at staff members. We realize that you are sick, that you feel lousy, and that dietary change is difficult, but it’s not our fault that you’re sick, and it’s not our fault that your genes are what they are. If you are upset about your genetic makeup, have a heated discussion with Charles Darwin or God (but they are not going to give in). Remember, just because we found an important problem that may be difficult to address, it doesn’t follow that we caused the problem.
It also doesn’t follow that we should work for free or lose money, just because we are the first practice in the area to provide Methyl Cycle testing and you have a lot of questions. Please remember, when a staff member takes your message, pulls your chart, brings the issue to my attention, and then transmit my answer back to you, a lot of staff time is taken up – and I am paying for it. We provide a lot of innovative services that generate a lot of questions, and the staff overhead generated can easily get out of hand.
If we are to continue to provide new and innovative services like Methyl Cycle testing, well, we are going to need your cooperation. Call us when you need to (and there will be times when you need to) but if a question can wait, please put it off until your office visit or until the next Methyl Cycle support group meeting.
James C. Roberts MD FACC 8/24/08
Sample Report - Child with Neurodevelopmental Challenges
|
Nutrigenomic Report for Child with Neurodevelopmental Challenges |
||
|
Methylation Panel Abnormalities for Genes with Characterized SNPs |
||
|
Gene Name |
Variation |
Finding |
|
COMT |
V158M |
OK |
|
COMT |
H62H |
OK |
|
COMT |
61 |
OK |
|
VDR |
Taq |
Homozygous (+/+) |
|
VDR |
Bsm |
OK |
|
MAO A - Slow |
R297R |
Homozygous (+/+) |
|
ACAT |
102 |
OK |
|
MTHFR |
C677T |
OK |
|
MTHFR |
3 |
OK |
|
MTHFR |
A1298C |
Heterozygous (+/-) |
|
MTR – “Always On” |
A2756G |
Heterozygous (+/-) |
|
MTRR |
A66G |
Homozygous (+/+) |
|
MTRR |
H595Y |
nc |
|
MTRR |
K350A |
OK |
|
MTRR |
R415T |
nc |
|
MTRR |
A664A |
OK |
|
BHMT |
2 |
Heterozygous (+/-) |
|
BHMT |
4 |
nc |
|
BHMT |
8 |
Homozygous (+/+) |
|
AHCY |
1 |
Homozygous (+/+) |
|
AHCY |
2 |
nc |
|
AHCY |
19 |
Homozygous (+/+) |
|
CBS |
C699T |
OK |
|
CBS |
A360A |
Heterozygous (+/-) |
|
CBS |
N212N |
OK |
|
SHMT |
C1420T |
nc |
|
Hormone and Toxin Metabolism |
||
|
CYP1A2 – Reduced Fn |
rs762551 |
Heterozygous (+/-) |
|
CYP1B1 L432V |
rs1056836 |
Heterozygous (+/-) |
|
CYP1B1 N453S |
rs1800440 |
Homozygous (+/+) |
|
|
Cardiovascular Genes |
|
|
NOS3 |
rs1800779 |
Homozygous (+/+) |
|
NOS3 |
rs1800783 |
Homozygous (+/+) |
|
|
Antioxidant Defenses |
|
|
SOD2 – Reduced Fn |
rs4880 A16V |
Homozygous (+/+) |
|
SOD2 – Reduced Fn |
rs2758331 |
Homozygous (+/+) |
|
CAT |
rs1049982 |
Homozygous (+/+) |
|
NQO1 |
Several |
Heterozygous (+/-) |
|
Glutathione Generation and Utilization |
||
|
GSTP1 I105V |
rs1695 |
Homozygous (+/+) |
|
GGT1 |
rs5751901 |
Heterozygous (+/-) |
|
|
Detoxification |
|
|
CYP2D6 S486T |
rs1135840 OK – Wild Type |
Heterozygous (+/-) |
|
CYP2C19*17 Fast |
rs12248560 |
Heterozygous (+/-) |
|
NAT2 Fast |
rs1208 K268R |
Heterozygous (+/-) |
|
NAT2 Slow |
rs1801280 |
Heterozygous (+/-) |
|
|
Toxin Sensitivity |
|
|
BDNF |
rs11030104 T64089C |
Homozygous (+/+) |
|
|
Additional Methyl Cycle |
|
|
DHFR |
rs1643649 |
Heterozygous (+/-) |
|
MTHFD1 |
|
Homozygous (+/+) |
|
MTHFS |
|
Heterozygous (+/-) |
|
PEMT |
rs4244593 |
Heterozygous (+/-) |
|
PEMT |
rs7946 |
Homozygous (+/+) |
|
GAD1 |
|
Homozygous (+/+) |
|
GGH |
rs3780126 |
Homozygous (+/+) |
|
MAT1A |
rs1985908 |
Heterozygous (+/-) |
|
CTH |
Several |
Heterozygous (+/-) |
|
TCN |
rs1801198 |
Heterozygous (+/-) |
|
|
Neurotransmitter Metabolism |
|
|
TH |
rs6356 |
Homozygous (+/+) |
|
GCH1 |
rs2878169 rs3783642 |
Homozygous (+/+) |
Overview
The function
of the Methyl Cycle is to maintain (current health status) appropriate levels
of:
A. SAMe, along with a high SAMe:SAH ratio, necessary for biological methylation.
B. BH4, need to generate neurotransmitters and nitric oxide.
C. The antioxidant/detoxification molecules cysteine, taurine, sulfate, and
glutathione.
D. Purine and Pyrimidine bases for DNA and RNA generation.
You are (+/-) heterozygous (½ of your CBS enzymes contain the variant allele) for the CBS A360A up regulation (up regulation refers to an abnormal increase in function) and (+/+) homozygous for one (all of your BHMT enzymes contain the variant allele) and (+/-) heterozygous for a second BHMT down regulation (which act like CBS up regulations). The nc designation means that 23and me could not genotype the third BHMT allele)
Thus, in a process that is exacerbated by chronic oxidative and/or inflammatory stress (your detoxification and antioxidant enzyme down regulations and recurrent infections predispose you to oxidative stress), homocysteine (and its Methyl Cycle precursors) is being irreversibly diverted down the trans-sulfuration pathway (why your homocysteine level is low at 4.7 despite MTHFR, MTR, and MTRR valiant alleles that are typically associated with an elevation in homocysteine) and away from useful remethylation into SAMe, in this process generating excessive sulfur break down products (sulfite and sulfate, which stimulate the stress/cortisol “fight or flight” response; your urine sulfate level has been as high as 1200), too much glutamate (which leads to glutaminergic excitotoxicity; and you harbor a genomic predisposition, GAD1 +/+, that impairs conversion of glutamate in to GABA, a calming neurotransmitter; toxic metals, particularly lead, also impair glutamate to GABA interconversion), too much hydrogen sulfide (leading to brain fog), and too much ammonia (which depletes BH4, which in turn may lead to insufficient dopamine and serotonin production).
Being +/+ for GTP cyclohydrolase (GCH1), you may also be having trouble generating BH4, and +/- status for DHFR (dihydrofolate reductase) may compromise recycling of oxidized or “spent” BH2 back in to useful BH4. Dr. Yasko feels (and other authors disagree with her position) that the MTHFR A1298C allele (you are +/- here) compromises the ability of methyl-folate to promote recycling of “spent” BH2 back in to useful BH4. In any event, with respect to the precious molecule BH4, you are likely getting hit at both ends; reduced supply and increased demand. After any problems in the trans-sulfuration pathway (CBS and BHMT) have come under control, BH4 or additional methyl-folate as a BH4 precursor/mimic could be added to your program.
Any deficiency in BH4 will predispose NOS (nitric oxide synthase) to convert arginine in to superoxide as opposed to nitric oxide, predisposing you to hypertension and cardiovascular disease later in life. Compounding this problem you are +/+ for two NOS down regulations, likely compromising nitric oxide generation and possibly ammonia detoxification.
Being +/+ for SOD2 (mitochondrial superoxide dismutase, which protects the energy generating mitochondria from the damaging effects of free radical superoxide), +/+ for CAT (catalase, which breaks down the hydrogen peroxide generated from superoxide by superoxide dismutase), and +/- for NQO1 (which neutralizes oxidized quinone molecule), you are having trouble neutralizing superoxide and other free radical molecules and thus you are predisposed to free radical accumulation and oxidative stress, phenomena that we can measure and address (your antioxidant defenses were at the 38th percentile – not expected at your age - and glutathione was low – it is being used up neutralizing free radicals and toxins).
CBS actually generates cystathione, which is rapidly converted by the P-5-P (active form of B6) dependent enzyme cystathionine gamma ligase (CTH) downstream to cysteine, and here you are somewhat compromised as you are +/- for a CTH down regulation.
CBS and CTH generate sulfite, which is converted in to less toxic sulfate by SUOX, an enzyme that becomes “overworked” and “co-factor depleted”. We can support SUOX function by supplementing you with its co-factors molybdenum, boron, Vitamin E succinate, and hydroxy-B12. Why supporting this pathway with molybdenum brings on incontinence is something that I cannot explain.
The high levels of sulfur break down products may (Dr. Yasko’s position) compromise the absorption of detoxifying sulfur based molecules (cysteine and glutathione) in to your cells, compromising endogenous detoxification (setting you up for organic pollutant and heavy metal overload).
Regarding toxicity, as you are +/+ for GSTP1 (glutathione-S-transferase) your ability to utilize glutathione in Phase II detoxification is compromised. Being +/- for GGT1, your ability to recycle glutathione may also be subpar. You are also +/+ for a reduced function allele of BDNF (Brain Derived Neuroprotective Factor) which defends the nervous system from toxins. You do not bear the CPOX4 mercury sensitivity allele (in your favor).
MTR uses 5-methyl folate and methyl-B12 to convert homocysteine in to methionine, which in turn is converted into SAMe (S-Adenosyl Methionine), the universal methyl donor (a key goal is to increase SAMe and your SAMe to S-Adenosyl Homocysteine ratio). You are +/- for the MTR up regulation, meaning that homocysteine recycling back to methionine (and SAMe) through the MTR pathway will be overly active and dysfunctional, predisposing you to methyl folate and methyl-B12 deficiency (which then would shut down MTR activity). MTR is also sensitive to inhibition by toxins, particularly mercury.
As you are
-/- (“wild type” or normal function) for MTHFR C677T, conversion of folic acid
(or more specifically 5,10-methylene THF) in to methyl-folate is not compromised
(your +/- status for MTHFR A1298C probably has little effect on this step).
Being +/+ for a MTRR down regulation, you are having trouble B12 in to
methyl-B12, a constraint that is easy to bridge with methyl-B12
supplementation. However, we will move slowly with methyl-B12 supplementation,
as spinning this limb of the Methyl Cycle forward (generating SAMe) can lead to
increased flow down the CBS pathway (aggravating a sulfite/ammonia/glutamate
overload state). This is why people with CBS up regulations may initially feel
poorly with B vitamin supplementation.
Folate molecules serve to transfer methyl groups within our physiology (think of
folates as “methyl group taxis”). To become useful, the oxidized dietary folate
molecules that we take in are first reduced to Tetrahydrofolate (THF) by
dihydrofolate reductase (DHFR), and here you are +/- for a DHFR down
regulation. Your folate receptor genomic status is intact.
SHMT (serine hydroxyl methyl transferase – here you are nc, meaning that 23and me could not, for technical reasons, genotype you at SHMT), like CBS a pyridoxal-5-phosphate dependent enzyme, tacks on a methyl group derived from the amino acid serine to generate 5,10-MethyleneTHF, which is then converted to 5-methyl folate by MTHFR. 5,10-MethyleneTHF can also be acted upon by MTHFD1,to generate the building blocks for DNA and RNA generation. Being +/- for MTHFD1, you may be having trouble with these steps and in recycling folates back into THF. Being +/+ for MTHFS, you are having some trouble breaking down folinic acid, which in turn inhibits SHMT. We can measure folate metabolites, and supplement you based upon the results, but these SNIPs are likely not important in individuals with adequate intake of folates, serine, and P-5-P (pyridoxal-5-phosphate, the active form of B6).
Why are you so B6 (the precursor of P-5-P) sensitive? Could it be that B6 is opening up flow through the Methyl Cycle, aggravating a sulfite/sulfate/glutamate/ammonia overload state?
MAT1A +/- status in theory compromise the conversion of methionine in to SAMe, but the expression (how they actually affect your physiology) of these SNIPs (single nucleotide interpositions – the genomic variations that we are discussing) is felt to be low (in any event the Drs. Data Methylation panel will give us levels of methionine and SAMe). You are +/+ for a reduced function allele of GGH (Folypolyglutamate synthase), which catalyzes the release of folates from intracellular storage, a constraint that we can address by optimizing methyl-folate status.
SAMe, generated by methylation of
homocysteine, gives up its methyl group to other molecules (its role within our
physiology; SAMe is the methyl donor in over 300 methyl group dependent
functions) and becomes S-adenosylhomocysteine (SAH), which is converted in to
homocysteine by AHCY. High levels of S-adenosylhomocysteine act to inhibit
SAMe-dependent interactions (it is not the absolute level of SAMe that drives
forward useful biological methylation, but rather the ratio of SAMe to SAH).
Being +/+ for at least two AHCY alleles, you are probably having trouble
converting S-adenosylhomocysteine in to homocysteine (and we can find out by
direct measurement of these biomolecules with the Drs. Data Methylation panel).
In this situation SAH levels will build up, the SAMe:SAH ratio will fall, and
biological methylation will be compromised.
Your low homocysteine level of 4.7
may thus be explained, at least in part, by:
A. Rapid metabolism down the CBS “drain”, and
B. Reduced generation from SAH due to your +/+ status for AHCY.
I predict that your SAH level will be elevated and your SAMe:SAH ratio low.
PEMT uses three SAMe molecules to generate phosphatidylcholine. You are +/+ for a loss of function PEMT allele, and thus you are having trouble generating phosphatidylcholine. We use phosphatidylcholine in the remethylation of homocysteine into methionine by BHMT (also pulling homocysteine away from the “CBS drain”), in lipid metabolism, and in the generation of the neurotransmitter acetylcholine. Phosphatidylcholine deficiency is one of the links between methyl cycle dysfunction and fatty liver.
We spend 2/3rds of our SAMe in the generation of phosphatidylcholine and creatine, and supplementation with these substances will spare SAMe for other more critical activities (such as maintaining proper DNA methylation and in the generation and break down of neurotransmitter substances). Thus if we find that SAMe is low or SAH elevated (as I suspect), we could add creatinine to decrease SAMe expenditure.
You are +/+ for VDR Taq, such that Vitamin D will be less efficient in generating dopamine (thus you might benefit from a Vitamin D level greater than your current 37), and -/- for COMT, meaning that you can breakdown dopamine rapidly, using up methyl groups in doing so, and thus you will have an increased susceptibility to toxic metals and viral infection. Conversely, your need and tolerance for methyl groups and methyl donors will be relatively increased.
MAO A breaks down serotonin (and to a lesser extent dopamine). You are +/+ for the MAO-A (rs6323) down regulation and this will compromise your ability to break down serotonin. MAO-B breaks down dopamine and norepinephrine (as does COMT), and here you are genomically normal (-/- or wild type). Overall your ability to break down serotonin will be reduced relative to your ability to break down dopamine.
Being +/+ for a TH (tyrosine hydroxylase, which generates dopamine form tyrosine) down regulation, dopamine generation will be compromised. Neurotransmitter generation requires raw materials (tyrosine for dopamine and tryptophan for serotonin), co-factors such as BH4 and SAMe, and intact enzyme function. Your +/+ status for GCH1 (and +/- status for DHFR and up regulated CBS pathway) may be compromising BH4 availability, and we suspect that your SAMe:SAH ratio (and thus ability to utilize SAMe) will be low.
To my knowledge, methylphenidate (Daytrana patch) acts as a dopamine “stand in”, suggesting that these SNIPS (which may compromise dopamine generation) are adversely affecting your health. The NutrEval will give us amino acid precursor and neurotransmitter metabolite levels and the Sanesco study will give us urine neurotransmitter levels.
You are +/+ for a GAD1 (involved in interconversion of glutamate into GABA) impaired function allele, setting you up for glutaminergic excitotoxicity, which we can address with GABA/Zen supplementation and dietary glutamate avoidance. Metal toxins also compromise this interconversion.
CYP2D6 metabolizes 20% of prescription drugs, and you do not bear any significant down regulations for CYP2D6. NAT2 metabolizes toxins via acetylation, and here you are +/- for both fast and slow versions of this enzyme. CYP2C19 metabolizes a number of psychotropic drugs. Your CYP2C19*17 +/- status is associated with somewhat increased metabolic activity of this enzyme (stated otherwise you are +/- for an up regulation).
TCN2 +/- status may compromise delivery of B12 to your cells, a constraint that is easy to overcome by optimizing B12 nutriture.
The Gene by
Gene sections provide generic information while specific recommendations for you
are described in the Plan of Action sections. I can and will be more definitive
after we obtain more information regarding your toxin burden and level of
expression of your CBS up regulation (and ideally with a NutrEval and urine
mineral assessment of your nutritional/oxidative stress/inflammation status and
a Drs. Data Methylation Panel measurement of SAMe and SAH).
We think of autism and other neurodevelopmental delays as an interaction between
environmental toxin exposure and genomic predisposition to impaired
detoxification and oxidative stress, aggravated by infection and GI tract
dysfunction. Your Methyl Cycle status serves as a predisposition. Your hair
analysis demonstrated a toxic burden. We expect this in older individuals, who
have had decades to accumulate toxins, but not in kids. Further analysis of
toxic burden and approaches to detoxification will be discussed.
My basic thoughts, based upon the information that you forwarded to me, follow. Please keep in mind that my background is Integrative Cardiology, not Pediatric Neurology or Infections Disease (areas where my knowledge will be limited). Obviously, we need to ensure that these recommendations do not conflict with the care that you are receiving from your other practitioners, who know your situation better than I do (maybe some of the steps that I recommend have already been taken). A supplement check list is attached (with supplement doses pertinent to adults). Approaches that make the most sense to me receive a (Ö). Those that are less critical (or more costly) are designated (+/-). I will be more definitive based upon results of the lab studies recommended below. Given your sensitivity to several supplements, my thought would be to start with doses below that which I recommend and to slowly advance the dose, watching for intolerance. Also, please add new agents one at a time. I have a number of additional thoughts beyond analysis of your genomic status, and I will start with these issues.
Gastrointestinal Tract
Dysbiosis (inappropriate mix of intestinal flora), and intestinal hyperpermeability (known as “leaky gut”), and SIBO (Small Intestinal Bacterial Overgrowth) may be present. We can evaluate you for these conditions with the GenovaLabs GI Effects comprehensive digestive stool analysis and with their SIBO test. These studies are not high on our “to do” list but are future thoughts.
MME and Magnetic Sleep Pad Therapy
We feel that a static magnetic field promotes detoxification. I have been sleeping on a 20 Gauss negative field only sleep pad over the past decade. MME (Magnetic Molecule Energizer Therapy) involves the application of a more powerful static magnetic field to the brain, heart, or other internal organ or body region. Electrical energy is transduced in to biological energy, assisting in cellular repair and detoxification. We have helped several kids with Autism by combining MME with their other treatments. Please review the attached DVD and look through our website. You could also contact Dr. Bonlie, the inventor of MME, for his thoughts. My personal patients (you would qualify) can obtain the sleep pads at a significant discount.
Hunt Digital Picture Analysis and Digital Patch Homeopathic Therapy
This approach is difficult to
explain and may be difficult to understand and accept. Our body emanates
frequency data that can be used to asses our internal physiology. Abnormal
patterns reflect internal disturbances, disturbances that can be rectified by
the use of homeopathic patch therapy. This has worked out well in medication
sensitive individuals and in Autistic kids. Please listen to Dr. Hunt’s audio
CD, which is enclosed (and consider where the “R” in R1H2 came from). A blank
report is attached, and discusses how patch therapy works. You can go to
www.auraexplorationpatches.com for additional information. The cost of the
digital picture analysis is $350 and the individual patches cost between $30-$40
for a one month supply.
“Peptide” Therapy
We utilize “false target” immune modulators to “call off” an inappropriate immune response. I have a five year experience with this approach in cardiovascular, auto-immune, and allergic conditions. A physician in N. Carolina has an extensive experience using this approach in Autism. Our information sheets on this approach are attached. Peptide therapy probably does not remove the underlying problem, but may lessen the symptoms of auto-immune involvement in Autism.
Gene by Gene Approach – CBS +/ and BHMT +/+ and +/-
CBS (Cystathionine Beta-Synthase) is discussed on pages 48-53 of Dr. Yasko’s book, Genetic Bypass. Additional information is available on our heartfixer.com website and within the attached material. You are +/- (½ of your CBS enzymes are abnormal) for the A360A CBS up regulation and you are +/+ (all of your BHMT enzymes bear the dysfunctional allele) and +/- for BHMT (which normally pulls homocysteine away from the CBS drain and back towards SAMe). Homocysteine (and its Methyl Cycle precursors) is thus being “pulled” by CBS and “pushed” by BHMT down the trans-sulfuration pathway, in this process generating excessive sulfur break down products (sulfite and sulfate, which stimulate the stress/cortisol “fight or flight” response), too much glutamate (which leads to glutaminergic excitotoxicity – a double problem for you as you are having (+/+) trouble converting glutamate to GABA), hydrogen sulfide (to produce brain fog), and too much ammonia (which depletes BH4, leading to insufficient dopamine and serotonin production). Your GCH1, DHFR, and MTHFR A1298C SNIPS may lead to reduced BH4 generation and recycling. Thus with respect to the precious molecule BH4, you are getting hit at both ends – reduced production and increased utilization.
A deficiency in BH4 will compromise neurotransmitter generation. A deficiency in BH4 will predispose eNOS (endothelial nitric oxide synthase, which in you may hypofunctional as you are +/+ for two NOS down regulations) to convert arginine in to free radicals (superoxide and peroxynitrite) as opposed to nitric oxide (atheroprotective vasodilator), predisposing you to hypertension and cardiovascular disease (later in life) and inflammatory disease states.
Thus your ability to generate neurotransmitters and nitric oxide will be compromised. Instead your genomic status predisposes nitric oxide synthase to generate the free radicals superoxide and peroxynitrite, which lead to oxidative stress and inflammation. Compounding this predisposition towards increased production of superoxide, your SOD2 +/+ status compromises your ability to neutralize (mitochondrial) superoxide and CAT +/+ status compromises your ability to neutralize peroxide generated from superoxide.
I realize that this sounds awful but these are all issues that we can deal with, now that we understand their origin and biological significance. Also, we need to realize that the vast majority of these genomic variants lead to enzyme activity that is only slightly greater or lesser than normal wild type (“wild type” is the term used to designate the most commonly encountered or “usual” genomic structure of a given enzyme or molecule).
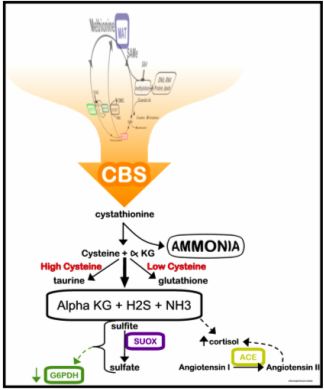 Within
our physiology, metabolic flow down the CBS pathway is designed to generate the
important anti-oxidant and detoxifying molecules glutathione, taurine and
cysteine (all involved in detoxification and endothelial health), and glutamate
(which can be converted into GABA, a calming neurotransmitter). The CBS C677T
and A360A genes code for enzyme function that is pathologically up regulated
(your ancestors needed antioxidant support more than they needed methylation
support; thus these SNIPs which direct homocysteine towards glutathione and away
from SAMe regeneration). Of the two, the C677T allele is the most important,
producing enzyme activity that is 10 fold greater than normal. Depending upon
the degree to which your CBS A360A up regulation is expressing itself, you may
suffer from “too much of a good thing and way too much of several bad things”.
Within
our physiology, metabolic flow down the CBS pathway is designed to generate the
important anti-oxidant and detoxifying molecules glutathione, taurine and
cysteine (all involved in detoxification and endothelial health), and glutamate
(which can be converted into GABA, a calming neurotransmitter). The CBS C677T
and A360A genes code for enzyme function that is pathologically up regulated
(your ancestors needed antioxidant support more than they needed methylation
support; thus these SNIPs which direct homocysteine towards glutathione and away
from SAMe regeneration). Of the two, the C677T allele is the most important,
producing enzyme activity that is 10 fold greater than normal. Depending upon
the degree to which your CBS A360A up regulation is expressing itself, you may
suffer from “too much of a good thing and way too much of several bad things”.
Oxidative stress (the accumulation of free radicals) increases flow down the CBS pathway, to generate the above listed antioxidants needed to allow the body to respond to an oxidative challenge – a good thing. However, when homocysteine is drawn down the CBS pathway, it is “lost forever” such that it cannot be remethylated and used to regenerate SAMe (could this be occurring in you?). In this fashion oxidative stress (which you are experiencing – your antioxidant defense and glutathione levels were low in 10/14) leads to reduced SAMe. SAMe itself stimulates flow down the CBS pathway (if you have plenty of SAMe you do not need to worry about recycling it); this is why we advise you not to begin SAMe until your CBS/BHMT alleles have come under metabolic control.
While sulfate and sulfhydryl (-SH) bearing molecules are important in detoxification, sulfate/sulfite/-SH excess seems to block cellular up take of the key detoxifiers glutathione and cysteine. Endogenous detoxification is thus blunted (nearly all kids with Autism Spectrum Disorders bear CBS up regulations – why they are compromised by environmental toxins and the kid next door is just fine – could this be playing a role in your otherwise difficult to explain health conditions)? Conversely, after we decrease your sulfate/sulfite pool, your detox pathways will open up (and why, if we move too fast, you will experience detox phenomena – could this explain your intolerance to B6 and molybdenum?).
The excess ammonia generated must be detoxified, and to do so BH4 (tetrahydrobiopterin) must be “spent”. This is a problem in that we need BH4 to generate neurotransmitters (serotonin to maintain calm/prevent depression and dopamine to maintain motivation and drive). Without BH4, we cannot convert arginine in to nitric oxide; instead vascular wall toxic free radicals such as superoxide and peroxynitrite are created, leading to hypertension and cardiovascular disease.
Ammonia is metabolized within the urea cycle, an enzyme pathway that utilizes several amino acids (ornithine, aspartate, arginine, and indirectly alpha-ketoglutarate) to break down ammonia. Systemic ammonia detoxification takes place in the liver, and thus individuals with advanced liver disease experience hyperammoniaemia, with attendant neurological dysfunction (tremor, confusion, impaired coordination). We can thus borrow from the gastroenterology community in our approach to the hyperammoniaemia present in our patients with CBS/BHMT/MTHFR alleles (also giving me a chance to consult with our daughter, who is a gastroenterology fellow).
Intestinal microbes generate ammonia. Gastroenterologists use antibiotic therapy (Rifaxamin, a poorly absorbed antibiotic that does not enter the circulation) to sterilize the gut, thus blunting ammonia production. While we may recommend antimicrobial therapy if bacterial overgrowth is demonstrated on a CDSA or SIBO study, a basic approach will be to take a probiotic 2-3 times a day to promote a balanced intestinal flora (not a bad idea for all of us to deal with the effects of antibiotics found in grocery store meats).
Why are you intolerant to probiotics? If one has SIBO (Small Intestinal Bacterial Overgrowth) then prebiotics (food for bacteria) could add to the burden but I cannot explain your intolerance to probiotics. Genova Labs provides a home test for SIBO.
Charcoal seems to absorb ammonia generated within the GI tract, and thus taking charcoal at bedtime seems to lower one’s ammonia burden (and charcoal also serves as a detoxification aide). Charcoal can also cause constipation, a huge negative here, as moving your bowels 2-3 times a day is important in detoxification and ammonia neutralization. Thus we recommend charcoal three nights a week with magnesium citrate and/or Vitamin C as needed to promote normal GI tract motility (adjust doses to obtain a balance between ammonia neutralization and proper GI tract function – too much magnesium or vitamin C pulls water into the intestines, leading to loose stools and diarrhea). Gastroenterologists utilize the cathartic lactulose to accelerate GI tract motility, blocking ammonia absorption; we can achieve the same end nutritionally with vitamin C and magnesium.
Ornithine/Aspartate supplementation (LoLa), administered IV or orally, has been shown to be a safe and effective approach to ammonia reduction in liver failure, and we can utilize this low cost approach to deal with ammonia excess in Methyl Cycle patients, starting with 1000 mg (1/3rd teaspoon) three times a day, increasing to one teaspoon as needed. Aspartic acid has a glutamate-like stimulating effect, and if one experiences agitation/anxiety than aspartate can be dropped in favor of more ornithine. Ornithine monotherapy has been used to increase exercise capacity in healthy people, as ammonia production is a metabolic consequence of energy utilization. These and other amino acids are best absorbed on an empty stomach or with a carbohydrate; concomitant protein intake will blunt their absorption.
 Dr.
Yasko’s diagrams indicate that CBS generates alpha-ketoglutarate, which can be
converted into glutamate. Actually, CBS generates alpha-ketobutyrate.
Nonetheless, individuals with CBS + alleles nearly always display elevated
glutamate, and thus the same physiology holds. We should be able to
interconvert alpha-ketoglutarate into glutamate, glutamine, and GABA (you are
genomically challenged here). However, if glutamate is in excess, or if
toxic metals compromise the interconversion enzymes, then we suffer a buildup of
the excitatory neurotransmitter glutamate. Glutamate is involved in alertness
and learning, but excess glutamate leads to irritability and over-excitement;
toxic levels may play a role in seizure activity and cardiac arrhythmia (could
this be why we are seeing so much more atrial fibrillation now then we were ten
years ago; MSG, a dietary source of glutamate, can precipitate atrial fib)?
Dr.
Yasko’s diagrams indicate that CBS generates alpha-ketoglutarate, which can be
converted into glutamate. Actually, CBS generates alpha-ketobutyrate.
Nonetheless, individuals with CBS + alleles nearly always display elevated
glutamate, and thus the same physiology holds. We should be able to
interconvert alpha-ketoglutarate into glutamate, glutamine, and GABA (you are
genomically challenged here). However, if glutamate is in excess, or if
toxic metals compromise the interconversion enzymes, then we suffer a buildup of
the excitatory neurotransmitter glutamate. Glutamate is involved in alertness
and learning, but excess glutamate leads to irritability and over-excitement;
toxic levels may play a role in seizure activity and cardiac arrhythmia (could
this be why we are seeing so much more atrial fibrillation now then we were ten
years ago; MSG, a dietary source of glutamate, can precipitate atrial fib)?
CBS up regulations lead to an initial buildup of potentially neurotoxic sulfite, which is then metabolized by SUOX (Sulfite Oxidase) to the less neurotoxic (but still problematic at high levels) sulfate. SUOX activity requires molybdenum, which is thus depleted in CBS + individuals. Homogenized dairy products contain xanthine oxidase, which uses up molybdenum, and are best avoided or minimized. Vitamin E succinate, boron, and B12 are felt to stimulate SUOX activity.
CBS is P-5-P (pyridoxal-5-phosphate, the active form of B6) dependent and utilizes serine as it converts homocysteine in to cystathione. Individuals with up regulated CBS activity are often deficient in serine and P-5-P, compromising other metabolic pathways. Thus serine and P-5-P supplementation may be in order (we will evaluate your need for supplementation with a NutrEval study).
As Methyl Cycle function is needed in the biosynthesis of Co-Enzyme Q10 and Carnitine, individuals + for CBS will likely be energy depleted, and here supplementation (in relation to your COMT/VDR status) with Co-Enzyme Q10, Carnitine, and NAD+ may be helpful.
BHMT (Betaine Homocysteine Methyl Transferase, a Zinc dependent enzyme – and Zinc supplementation is already on board) directly methylates homocysteine back in to methionine, serving as a “back door” pathway to “pull” homocysteine away from the CBS “sulfate drain”. Thus if you bear CBS or BHMT abnormalities, it makes sense to support BHMT function. TMG (trimethylglycine) stimulates BHMT, and can be utilized if you are not overly sensitive to methyl group supplementation (and you are probably not methyl donor sensitive as you are VDR +/+ and COMT -/-). Phosphatidylserine (already on board) stimulates BHMT (and we also use it to moderate elevated cortisol levels), as does phosphatidylcholine (which we use to treat atherosclerosis, liver, and neurologic dysfunction). Phosphatidylcholine can be admixed with EDTA (detoxifies metals), creating a quite useful supplement (and you are having some trouble generating phosphatidylcholine due to your PEMT +/+ status). You are taking DMAE, a choline precursor and methyl donor. I am less familiar with DMAE but my understanding is that it will support the BHMT pathway.
Many of you with CBS and BHMT abnormalities will also bear MTHFR (compromising methyl-folate generation) and MTRR (compromising methyl-B12) abnormalities, and thus you will need and benefit from corresponding supplementation (with these molecules that you are having trouble making). However, if we supplement heavily with methyl-folate, methy-B12, or BH4, before we have the CBS/BHMT physiology under control (until we have reduced your sulfate status such that glutathione and cysteine assimilation improves) then we will be subjecting you to a “sulfite surge”. You will feel great for 1-2 days, as beneficial neurotransmitters are generated. Methyl-folate and methyl-B12 detox pathways will then open up, creating toxic intermediates that cannot be metabolized further due to the block in glutathione utilization – and you will feel horrible. Thus we need to resist the temptation to treat your MTHFR/MTRR abnormalities until CBS/BHMT are under control. You’ve lived your entire life with a gene set that is maladaptive to the toxic environment of modern man. It will take us some time to change your internal environment to “bypass” these genomic challenges.
Plan of action for CBS +/- (BHMT discussed further in other sections)
Your genomically up regulated trans-sulfuration (CBS/BHMT)
pathway is likely important but it may not be your dominant health issue.
Additional testing (outlined below) will tell us how hard we need to push with
the CBS recommendations (given below) and to what degree you should (or should
not) restrict dietary animal protein. We can measure urine sulfate and
determine urine ammonia, glutamate, taurine, and cysteine within the Genova Labs
NutrEval study. If they are elevated, than the following steps will be
important. If not, then we can push further with Methyl Cycle supplementation
and detoxification.
1. Moderate animal protein* (anything with eyes) in your diet and avoid sulfur
rich vegetables, sulfur containing supplements, and sulfur containing drugs (see
Appendix II regarding high sulfate foods and supplements) and read Sulfites
and Chronic Disease by Rick Williams, available at the office or at
www.readingtarget.com/nosulfites/. The degree of protein/sulfur based vegetable
restriction will be based on your urine sulfate and ammonia levels, and how you
feel. We do not want a low protein diet to become a high carbohydrate, weight
gain diet that leads to insulin insensitivity. Stated otherwise, lowering urine
sulfate is not our only goal. Right now you seem to be on a quite
appropriate diet.
2. Check the sulfate/sulfite content of your supplements and prescription
agents (many listed in the Williams book) and whenever possible switch to agents
with lower sulfate/sulfite content.
3. Monitor urine sulfate levels every 3-7 days (or when you feel
particularly good or poorly, or after adding a new treatment or changing your
diet). Please chart the levels – this will be our primary measuring
stick – our goal is a urine sulfate of 400 (one yellow and three pink) to
800 (two yellow and two pink). Low levels will allow an increase in methyl
cycle supplementation and later the addition of BH4 and/or a liberalization of
your diet. Conversely, persistent high sulfate spills indicates that your
diet/treatment program needs further modification.
3. To neutralize ammonia (generated from animal protein), you can use Ammonia
Support RNA ½ dropper with meals and with methyl cycle supplements (relatively
expensive and thus elective), along with a charcoal supplement at bedtime
every other evening, away from other supplements (magnesium citrate and
Vitamin C may be used as needed to keep the GI tract moving - optimally twice a
day - as charcoal may lead to constipation). Yucca, beginning at ½ capsule,
twice a day, (or sprinkled on food containing protein), may help with ammonia
detoxification (I was not aware of the issue with testosterone).
Probiotic supplementation makes sense (but you do not tolerate probiotics).
Ornithine/Aspartate 1000-3000 mg three times a day (taken away from other
sources of protein) will stimulate the urea cycle, promoting ammonia
degradation, and should increase your energy level. Dr. Yasko’s CBS RNA
product, to my understanding (which may be incorrect), is an interference RNA,
which blunts the production of CBS. I’m not exactly sure of the biochemistry
here and as these products are relatively expensive I do not emphasize the RNAs,
but you can try them and see if they help. You thus have the option of adding
her CBS Support and Ammonia Support RNA products to your program (in theory this
would allow you to take in more animal protein with less homocysteine “spillage
down the CBS pathway).
4. Sparga Detox, 2-5 drops in water (wait at least one minute before
consuming), twice a day makes sense. Sparga was developed by fellow
Cardiologist Dr. Lee Cowden, specifically to address the CBS abnormality (see
www.nutramedix.ec). Right now you are taking 2 drops twice day. You can slowly
increase the dose and see what affect this has on urine sulfate and how you
feel.
5. Regarding nutritional support, I will provide specific recommendations after
your 24 hour urine mineral and Genova NutrEval studies have returned. To
stimulate SUOX activity, we use sublingual hydroxy-B12 2000 mcg/day (this
will also help with methyl-B12 generation) and Vitamin E Succinate 400 IU/day,
along with Molybdenum and Boron. In an adult, they may be taken individually as
Molybdenum 500 mcg/day and Boron 3 mg once a day, while the Designs for Health
Complete Mineral Complex, 3 daily will cover the mineral base (given your
size, one Complete Mineral Complex should suffice for you, and hopefully this
low dose of molybdenum will be adequately tolerated – if not you could omit
molybdenum and add boron 1 mg/day) If you begin Vitamin E succinate you
could decrease your current Vitamin E to 400 IU once a day – what type are you
taking, mixed tocopherols or alpha-tocopherol?).
6. Glutathione supplementation runs the risk off adding to your sulfite/sulfate
burden. Right now this “good thing” could actually set you back. However, if
we could convince your biochemistry to up regulate biosynthesis of glutathione,
then your anti-oxidant and detox capacity will increase, with concomitant
utilization of free sulfate/sulfhydryl groups – a double win for you. This can
be achieved with the use of the Life Wave (needleless acupuncture) Glutathione
patch. The Life Wave people have demonstrated an increase in Glutathione levels
in relation to patch use (please see separate information sheet on Life Wave
patch use). This should be put off until we feel you are ready for more
aggressive detoxification.
7. If you feel anxious or “wired up” (glutamate overload), take Zen (GABA
275 mg plus Theanine, a methyl donor, 100 mg) twice a day. If this is helpful
you can double the dose. GABA does not work rapidly, but if you take it twice a
day you will build up a GABA reserve to balance any glutamate overload you might
experience on the basis of your CBS up regulation. Magnesium supplementation
(Metagenics Mag Glycinate 100 mg 1-2 twice a day) may help with GABA physiology,
often helps with sleep, and maintains GI tract motility (evacuating your bowels
three times a day would be ideal and magnesium helps here; if it helps too much
than back down on the dose). You have this base covered with GABA and
magnesium; Zen is a better fit for your genotype but if all is going well there
is no need to change.
8. If NutrEval testing suggests impaired energy generation/mitochondrial
dysfunction, we could add Co-Enzyme Q10 (Ubiquinol) 50 mg, carnitine 500 mg, and
NAD+ daily. Ribose 5 gm two to three times a day may give you energy lift; if
so this would point to a problem in mitochondrial ATP energy generation
(possibly on the basis of toxin accumulation). Low energy does not seem to be a
problem for you right now.
9. With respect to lab testing, A Genova Labs NutrEval study ($170) and a
Doctor’s Date 24 hour urine mineral assessment ($60) will help us understand the
functional significance of your Methyl Cycle alleles, and will provide
information regarding oxidative/inflammatory stress, and give us Co-Enzyme Q10
and glutathione levels. We need to make sure your mineral/nutritional
stores are replete and we are looking at the levels of ammonia, taurine,
glutamate, and cysteine, to gauge the degree to which your CBS/BHMT SNIPs are
expressing themselves within your physiology. A Sanesco study ($90) will
give us salivary cortisol values and urine neurotransmitter (serotonin,
dopamine, etc.) values. The Health Diagnostics and Research Institute
(www.hdri-usa.com) can give us levels of SAMe, SAH, and folic acid derivatives
and this information will be helpful ($325). Doctors Data gives us a less
extensive but quite useful Methylation Panel for $155 (number one on our
list as we need to see what affect your AHCY +/+ status has on your SAMe:SAH
ratio). Toxicity testing** will be important later. I will rank the proposed
studies in order of importance (please see Intraoffice Work Sheet). They do not
all need to be done at once.
10. After sulfate levels have fallen (to a level that you and I feel is optimal
for you, based upon your clinical and genomic status), then we may advance
supplementation with methyl-folate, methyl-B12, and BH4. This will take some
time.
11. Sauna therapy increases BH4 production and promotes detoxification, and
could be utilized (low exposure at first, watching for detox reactions).
Footbath therapy is another means of removing toxins without adding foreign
molecules to your body.
12. Be self-observant and keep records. Which foods, supplements, or other
maneuvers increase or decrease your sulfate spill? Which make you feel better
or worse? Always keep in mind that detoxification is not a fun experience. You
may need to accept some transient fatigue, malaise, and achiness to allow toxic
molecules to be cleared. Conversely, if detox symptoms are debilitating or
compromise your ability to work or care for your family, then we need to back
off on your treatments. Balance needs to be achieved. Rectifying your genomic
predispositions and detoxifying your system is not a sprint – it is a marathon.
And, as your genes are not going to change, and as the environment is not going
to become less toxic, you will need to be mindful of these principles for the
rest of your (long and healthy) life.
* How tightly should you restrict dietary protein? The degree of protein restriction best suited for you will be in relation to your personal health characteristics and your clinical and biochemical (urine sulfate and ammonia levels) response to treatment. We need to keep in mind that Methyl Cycle Genomics is not the sole determinant of your health. A low protein diet can become a high carbohydrate, weight gaining diet in an overweight individual with metabolic syndrome or adult onset diabetes. Individuals with chronic, unexplained illness or significant toxicity would do well to follow the “nothing with eyes” diet until urine sulfate and ammonia levels have fallen; later on we will liberalize your diet, while keeping an eye on these biochemical markers. This maneuver isn’t fun and will require personal commitment, but it also may turn your health around. Individuals in whom the CBS up regulation is less important (A360A as opposed to C677T, lower urine sulfate and ammonia levels, and better overall health), could simply cut back on animal protein. In addition, the greater representation of ammonia reducing (Yucca, Charcoal, Sparga, Ammonia Support RNA) treatments in your program, the more protein you will be able to take in without compromising your biochemistry. This is all about balancing diet against treatment response.
** A key goal of Nutrigenomic Analysis is to help you
become a more efficient detoxifier. Toxicity testing (discussed in more detail
in other presentations and on heartfixer.com) thus makes sense. This could take
the form of:
A. The NutrEval provides us some information regarding organic pollutants and
gives us red cell (reflecting what your physiology has been exposed to over the
preceding three months) toxic metals ($170 with commercial insurance; fully
covered under non-HMO Medicare).
B. The US BioTek study gives us information on seven major organic pollutants
($126).
C. A formal provocative challenge (with IV/po chelators or po DMPS) gives us our
best assessment of tissue metal burden. Individuals with CBS up regulations may
feel poorly with DMPS, but this not the rule and any malaise would be short
lived. My hunch is that toxicity is a key underlying problem for you.
Autism/Developmental Delay was not present when I was growing up. Today the
rates are high and climbing rapidly. My feeling is that environmental toxicity,
interacting with one’s genomic predisposition to impaired detoxification, is the
explanation. We will put off formal metal toxicity testing until we have had
the opportunity to optimize your nutritional status (and the NutrEval and US
BioTek study will give us some information here) but toxicity testing will be
important in your evaluation.
D. The Hunt Digital picture approach ($350 – discussed previously)
assesses for toxicity (and other health challenges) by analyzing the frequencies
emitted by your body (and tells us which Digital Homeopathic Patches would be
most appropriate). I can’t prove this approach with an allopathic lab test but
it has been quite helpful in solving complex medical problems in my personal
patients. I often find unsuspected chronic infection that responds to
corresponding homeopathic therapy. Dr. Hunts CD is available for your review
and you can go to www.auraexplorationpatches.com for additional information.
They have digital patches to treat a number of chronic infections, including
Lyme. Many of my personal patients have benefitted from this approach. My staff
can coordinate this approach with you if you wish.
E. While on the subject of energy medicine, please learn about the
grounding/earthing concept. This approach is low in cost and likely has value
for all of us. My colleague Dr. Sinatra wrote a book on this subject
(heartmdinstitute.com).
F. A negative field only sleep pad (discussed earlier) enhances detoxification
and synergizes with oral metal chelators (I’ve been sleeping on one for 10
years). For more information please go to magneticosleep.com (as you are
working with me you would get 1/3rd off the list price). These pads
are expensive but they will last for 80 years.
AN IMPORTANT INITIAL GOAL WILL BE TO
REDUCE YOUR SULFATE, AMMONIA, and GLUTAMATE BURDENS
Gene by Gene Approach and Plan of Action – AHCY +/+
You are +/+ for two reduced function alleles of S-Adenosylhomocysteine Hydrolase (AHCY; sometimes referred to as SAHH). Thus you will have trouble converting SAH (created when SAMe donates a methyl group) in to homocysteine and adenosine. In this situation SAH levels will build up, the SAMe:SAH ratio will fall, and biological methylation will be compromised.
Your Drs. Data Methylation panel will tell us how this allele is affecting you. Keeping homocysteine on the low side should speed up AHCY activity. In theory, lowering adenosine should speed up SAHH activity. Ribose 5 grams three times a day (discussed in CBS section) might help here. Caffeine blunts adenosine breakdown as is best minimized (and you have trouble breaking down caffeine due to your CYP1A2 +/- status).
Gene by Gene Approach – COMT -/- with VDR Taq +/+, MTR +/-, and MTRR +/+
This constellation of alleles is discussed on pages 116-119
of Dr. Yasko’s book, Genetic Bypass. Additional information is available on our
heartfixer.com website. VDR Taq influences dopamine production. Being +/+ for
VDR Taq means that dopamine production is compromised (TH and GCH1 +/+ status
and presumed low SAMe:SAH may also compromise dopamine generation). Being COMT
-/- means that you are breaking down dopamine rapidly and in doing so using up
available methyl groups, compromising your ability to deal with toxins and
microbes (thus you are more likely than COMT +/- or COMT +/+ individuals to bear
a metal burden). You need and should tolerate dopamine precursors and methyl
donors.
COMT (Catechol-O-Methyl Transferase) inactivates catecholamines (dopamine,
norepinephrine, and epinephrine). Caffeine and stress increase catecholamine
production. Individuals with genomic or acquired COMT dysfunction are thus more
sensitive to their effects. Stated otherwise, high coffee intake increases
cardiovascular risk in COMT +/+ individuals but not in those with normal COMT
status, and caffeine induced insomnia will be more of an issue in those with
COMT +/+ than COMT-/- status. COMT is also involved in estrogen metabolism,
mediating generation of the anti-cancer, anti-vascular disease 2-methoxy
estrogens (see Estrogen Metabolism section of website) and inactivation of the
stronger, potentially genotoxic 4-hydroxy and 16-hydroxy estrogen molecules.
Endogenous and caffeine induced catecholamines, estrogen molecules, and
quercetin “compete” for COMT mediated methylation. This is not an issue in COMT
-/- individuals, as there is plenty of COMT function to go around, but when COMT
function is limited (COMT +/+ individuals have only 25% the O-methylating
capacity of COMT -/- individuals), competition becomes more of an issue. This
explains how stress and caffeine increases risk of cardiovascular disease and
reproductive organ malignancy to different degrees in different people
(genomic-environment interaction). While estrogens, quercetin, and
catecholamines “compete” for the attention of COMT, S-Adenosyl Homocysteine
(SAH) serves as a “non-competitive” COMT inhibitor. S-Adenosyl Methionine
(SAMe) donates the methyl group that COMT uses to O-methylate its substrate,
producing an O-methylated substrate and SAH. SAMe and SAH compete for the SAMe
binding site on the COMT molecule (think of the SAMe binding site as the
“on-off” switch for COMT). A build up of SAH will thus turn down COMT
activity. When Homocysteine builds up, SAH builds up behind it. COMT metabolic
dysfunction, with secondary inability to metabolize catecholamines and estrogen
molecules, is a key mechanism through which elevated homocysteine damages our
health. Unmetabolized catecholamines and estrogen molecules generate oxidative
stress, leading to vascular and neurological disease. Oxidized estrogen
molecules damage DNA, increasing risk of breast and prostate malignancy. While
elevated Homocysteine is always deleterious to overall health, high Homocysteine
in the presence of COMT dysfunction is a metabolic disaster. Your COMT
pathway is genomically normal and your homocysteine level is low. However, a
buildup of SAH due to your AHCY +/+ status could compromise COMT activity.
MTR uses 5-methyl folate and methyl-B12 to convert homocysteine in to methionine. The MTR A2756G abnormality is an up regulation, such that MTR is “always on”. Being +/- (half of your MTR enzymes are up regulated) for the MTR up regulation, you are over rapidly using up methyl-folate and methyl-B12 in the conversion of Homocysteine back into methionine, potentially depleting your methyl-folate and methyl-B12 reserves. The MTRR +/+ abnormality means that you are having difficulty converting B12 in to methyl-B12. You will thus likely be deficient in methyl-B12. As you are COMT -/- and VDR +/+, and thus not sensitive to methyl group supplementation, this deficiency is biochemically easy to overcome with methyl-B12 supplementation.
COMT -/- individuals can utilize methyl groups efficiently, and thus methyl group supplementation is not likely to lead to irritability (as it might in COMT +/+ individuals). Dr, Yasko feels that VDR status effects dopamine generation. As you are COMT -/- and VDR +/+ you should tolerate methyl group supplementation well. Stated otherwise, as you are COMT -/- and VDR +/+, you are making less dopamine in response to Vitamin D and you are breaking dopamine down rapidly. Thus you need and should tolerate methyl donors such as Methyl-B12, TMG, melatonin, curcumin, SAMe, or MSM (the only caveat here is that if urine sulfate is high, additional methylated B vitamin, SAMe, and MSM may tip you into a sulfite/sulfate excess situation – thus we do not wish to push here until urine sulfate levels are under control). If dopamine levels are low (we can check urine dopamine with the Sanesco study), you might benefit from quercetin (inhibits COMT) or macuna puriens (raw material for dopamine), or the Sanesco Procite-D preparation.
By stimulating BHMT, we can bypass any block that MTRR places on homocysteine detoxification, and this maneuver will also draw methyl cycle intermediates away from sulfate/sulfite production. Trimethylglycine directly stimulates BHMT, and its use makes sense. BHMT is zinc dependent (you are already taking zinc). PhosChol provides phosphatidyl choline which stimulates BHMT. DetoxMax (Lipophos EDTA) provides phosphatidyl choline to stimulate BHMT and EDTA to remove lead (which compromises function of multiple enzymes, whether they are genetically normal or abnormal, including GAD, which converts glutamate in to GABA) and cadmium (which contributes to hypertension and cancer risk).
If you are troubled by agitation or anxiety (perhaps on the basis of excessive glutamate production due to a CBS up regulation), we can address this with GABA or Zen (GABA plus Theanine). As you are COMT -/- and VDR Taq +/+, you should tolerate and benefit from the methyl groups provided by theanine. However, if agitation occurs, suggesting methyl group excess, we can utilize GABA, which does not contain methyl groups (both GABA and theanine stimulate the GABA receptor, and thus provide a “Valium” like effect without concern for drowsiness or dependency). Neither GABA or Zen work quickly (we have other supplements for “as needed” use) and are best taken twice a day as a nutritional approach to combat the biochemical consequences of stress (emotional or glutamate-induced stress). Other approaches to dealing with an imbalance between glutamate and GABA include avoiding glutamate rich food products (see appendix III) and supplementation with grape seed extract 100 mg/day and/or (if a CBS up regulation is not present) taurine 500 -1000 mg/day. DetoxMax (Lipophos EDTA) provides phosphatidyl choline to stimulate BHMT and EDTA to remove lead (which compromises function of multiple enzymes, whether they are genetically normal or abnormal, including GAD, which converts glutamate in to GABA). EDTA efficiently removes lead and cadmium, and has activity against aluminum, nickel, and arsenic. EDTA is not an efficient mercury chelator. EDTA is typically well tolerated in individuals with a CBS up regulation.
Plan of action for COMT -/- with VDR Taq +/+, MTR +/-, and MTRR +/+
1. Hydroxy-B12 is already on board to stimulate SUOX. If
methionine or SAMe are low on your Methylation panel we will add in methyl-B12,
starting at 500 mcg/day and advancing at weekly intervals to 2000 mcg/day (you
could start this now if you wish; intolerance is not likely – a sample bottle of
QuickSilver Methyl-B12 spray is enclosed).
2. Phosphatidylcholine (PhosChol 900 mg/day as a gel cap or liquid – both
available on-line) to stimulates BHMT and spare SAMe (much of our SAMe is
“spent” generating phosphatidylcholine) makes sense, particularly as your +/+
status for PEMT compromises endogenous production of phosphatidylcholine.
Later, if we feel that metal detoxification is appropriate we could switch to
low dose Lipophos EDTA (removes lead, cadmium, and aluminum). Please add ½ of a
TMG 750 mg once a day to directly stimulate BHMT; if this is well tolerated you
can increase to 750 mg daily (OK to wait until your SAMe and SAH levels return
but there are no down sides of TMG or phosphatidylcholine supplementation with
respect to your Methyl Cycle genotype.
3. A Sanesco study will give us urine dopamine (and other urine
neurotransmitter) levels and will tell us if dopamine support is needed.
4. If dopamine is low (and I suspect it is), we could intervene with:
A. Quercetin Plus, to blunt dopamine degradation by COMT.
B. After one to two weeks of Quercetin Plus we could add Sanesco Procite-D.
C. Depending upon your response, we could later add SAMe 200 mg/day or Sanesco
Methyl Max, and later we could add BH4 2.5 mg/day – a step-by-step approach
makes sense here.
5. We know that your Vitamin D status is OK at 37 and you are on a D supplement
(and we can recheck Vitamin D with your nest round of
labs).
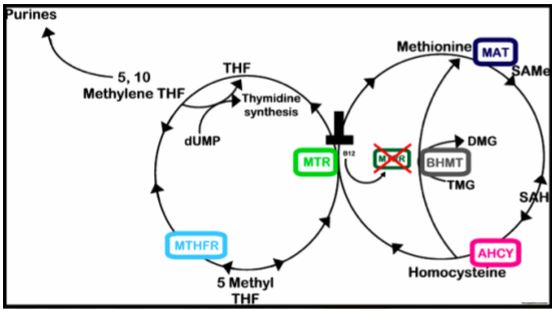
MTR (Methionine Synthase) transfers a methyl group from Methyl-folate to Homocysteine to form Methionine. MTRR (Methionine Synthase Reductase) adds the Methyl group to otherwise inactive B-12. MTRR abnormalities compromise the generation of methyl-12. Without methyl-B12, MTR cannot use methyl-folate to recycle homocysteine into methionine.
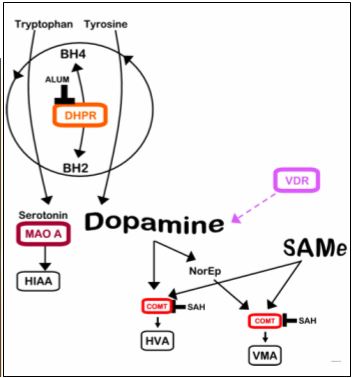
VDR Taq status compromise the production of dopamine. COMT -/- (normal function) allows rapid breakdown of the dopamine you can generate. VDR Taq+/+ with COMT -/- individuals will experience low dopamine levels (with consequent increased sensitivity to metal overload) and will benefit from dopamine precursor therapy and from methyl group donors.
Gene by Gene Approach – MTR2756G +/-
The MTR A2756G defect (also discussed above) is described by Dr. Yasko as an up regulation (other researchers call this a down regulation; either way, remethylation of homocysteine to methionine is compromised). MTR will thus be “always on”, potentially depleting your stores of methyl-folate and methyl-B12, aggravating any tendency you have towards methyl-folate and methyl-B12 deficiency on the basis of your MTHFR C677T and MTRR abnormalities. Of note, MTR activity is stimulated by dopamine and strongly inhibited by mercury.
Folate Processing Genes
Gene by Gene Approach – MTHFR A1298C +/-
Dr. Yasko describes MTHFR A1298C as an abnormality in the SAMe binding site of MTHFR that compromises the “backward reaction” that generates BH4, a problem in that BH4 is being used up detoxifying ammonia (which you may be making in excess due to your CBS up regulation). This “backward reaction” is not supported by other authors, but a pathway does exist (mediated by DHFR) such that poor methyl-folate status will compromise BH4 recycling. Methyl folate supplementation may stimulate the backward reaction and will help regenerate BH4, and methyl-folate can “stand in” for BH4 when the latter is depleted. After your urine sulfate levels have fallen we may advance methyl-folate or add in BH4 supplementation. If we supplement aggressively in the presence of high urine sulfate, patients may feel great for one day and then experience an incomplete detox reaction. Sauna increases BH4 production and promotes detoxification and could be utilized.
Gene by Gene Approach – DHFR +/-
Here you are having some trouble reducing oxidized dietary folates into useful Tetrahydrofolate, and in recycling “spent” BH2 back in to useful BH4. Our approach here involves methyl-folate and folinic acid supplementation.
Gene by Gene Approach – MTHFD1 +/+_
The trifuncitonal enzyme, 5,10-methylenetetrahydrofolate dehydrogenase/ 5,10-methylenyltetrahydrofolate cyclohydrolase/ 10-formyltetrahydrofolate synthetase (MTHFD1) is responsible for the conversion of 5,10-methylene THF (generated from THF by SHMT) to the corresponding 10-formyl, 5,10-methenyl and 5,10-methylene derivatives. The Health Diagnostics and Research Institute (www.hdri-usa.com) can give us levels of SAMe, SAH, and folic acid derivatives (which will help us understand the affects of your MTHFD1 and MTHFS alleles) but is rather expensive at $350.
Gene by Gene Approach – MTHFS +/-
Methenyltetrahydrofolate synthetase catalyzes the transformation of 5-formyl-tetrahydrofolate back to 5,10-methenyltetrahydrofolate, which is the obligatory initial metabolic step prior to the intracellular conversion of reduced folates into useful biological intermediates. Being +/- for MTHFS, you are having some trouble breaking down folinic acid, and a buildup of folinic acid can inhibit SHMT. Our approach here involves general support of the Methyl Cycle and the inclusion of methyl-folate and folinic acid in to your program.
Gene by Gene Approach – GGH +/+
Folate molecules are stored within our cells as polyglutamates. Folypolyglutamate synthase catalyzes the breakdown of folate polyglutamates to their monoglutamate forms, such that they can be released from intracellular storage for metabolic use. The GGH +/+ SNIP codes for reduced function of this enzyme. We address GGH +/+ be optimizing methyl-folate status.
Plan of Action– MTHFD1 +/+, MTHFS +/-, DHFR +/-, GGH +/+, and MTHFR A1298C +/-
The Health Diagnostics and Research Institute (www.hdri-usa.com - $350) can give us levels of SAMe, SAH, and folic acid derivatives (which will help us understand the affects of your MTHFD1 and MTHFS alleles) but is rather expensive at $350. A more practical approach is to supplement with methyl-folate and later folinic acid, after urine sulfate levels have fallen. Two weeks after B12 supplementation has been added, if urine sulfate remains £ 800, please add 400 mcg of methyl-folate/day to your program and two weeks later, if all is going well add in 400 mcg of folinic acid/day. You could start this program now or wait until your other diagnostic studies return.
Gene by Gene Approach and Plan of Action – MAT1A +/-
This SNIP, in theory, will compromise the conversion of methionine in to SAMe. The functional significance of these SNIPs appears to be limited. However, if our evaluation reveals high methionine and low SAMe, then we will bypass these SNIPs with direct SAMe supplementation.
Gene by Gene Approach and Plan of Action – CTH +/-
CTH (cystathionine gamma ligase), like CBS and SHMT a P-5-P (active form of B6) dependent enzyme, converts cystathione generated by CBS downstream to cysteine. The “penetrance” or functional significance of this down regulation is not certain. Our approach here is to make sure that P-5-P nutriture is optimal. Given your prior intolerance to B6 we will hold off on supplementation until your NutrEval results are available. My hunch is that your intolerance symptoms represent detox phenomena.
Gene by Gene Approach and Plan of Action – TCN2 +/-
This SNIP of Transcobalamin (B12 transporter), to some degree, compromises B12 transport. Our approach here is to optimize B12 nutriture and this base is covered in your program.
Antioxidant and Glutathione Genes
Glutathione Physiology – Gene by Gene Approach
GSS (Glutathione Synthase – here you are genomically normal or
“wild type”) generates glutathione and GSR (Glutathione Reductase – here you are
genomically unimpaired) recycles oxidized or “spent” glutathione. GGT (here you
are +/- for a reduced function allele) is also involved in glutathione
recycling. Thus you are having no trouble generating and just a little
difficulty recycling the key antioxidant and detox molecule glutathione. Your
low glutathione status is thus likely due to an increased demand for
glutathione, due to a toxic burden.
GPX1 (Glutathione Peroxidase), acts like Catalase, converting hydrogen peroxide derived from superoxide in to water (you are genomically normal for GPX1).
GSTP1 (here you are +/+ for a down regulation) utilizes glutathione in detoxification. Thus you are having significant difficulty utilizing glutathione as an antioxidant and in detoxification. Glutaclear, Protandim, and other agents that enhance NRF-2 translocation will increase generation of these enzymes. We can also treat you with topical, sublingual, or liposomal oral glutathione. We can combine glutathione with the metal binder DMPS in a topical format. The Life Wave glutathione patch is another approach to consider. Removing toxins will indirectly alleviate these genomic predispositions to impaired glutathione utilization. These enzymes are selenium dependent so maintaining adequate selenium nutriture is important (already on board).
Glutathione Physiology – Plan of Action
A NRF-2 translocator and Glutathione supplementation makes sense when we feel you are ready for more aggressive detoxification
SOD2 A16V +/+ and SOD2 rs2758331 +/+ Gene by Gene Approach
These are reduced function SNIP for mitochondrial,
manganese-dependent Superoxide Dismutase, which neutralizes the free radical
superoxide. Superoxide is generated as a byproduct of energy metabolism and
normal physiology, and at high levels in response to (real or perceived)
infection. If not neutralized by SOD (which converts superoxide in to hydrogen
peroxide), superoxide will initiate a damaging free radical cascade. GliSODin
is a nutritional supplement designed to up regulate superoxide dismutase
activity; this agent has been shown to have a favorable affect on carotid artery
IMT progression (which reflects your propensity to form plaque). GliSODin can
be obtained at health food stores or via Life Extension (lef.org). GliSODin is
patented and any product you obtain with this label will be OK. Sulforaphane
containing agents such as Metagenics Glutaclear will increase production of SOD
and other antioxidant and detoxification molecules. The NutrEval study will
tell us more regarding your level of oxidative stress (my prediction is that it
will be elevated). The standard dose of GliSODin is 250 mg twice a day (rather
expensive – once a day would be OK).
Gene by Gene Approach – CAT +/+
Catalase and Glutathione Peroxidase both break down hydrogen peroxide that is generated from superoxide by SOD. As you are +/+ for CAT, this step is compromised. CAT SNIPS have been associated with impaired weight maintenance and increased sensitivity to lead with respect to blood pressure elevation. Antioxidant support should neutralize CAT SNIPs. Metagenics Glutaclear or the Protandim preparation will increase generation of antioxidant and detox molecules. If measures of oxidative stress (lipid peroxides, 8-OHdG, oxidized LDL, and glutathione) return abnormal, then supplementation would be in order. The CAT SNIPS that you bear are not discussed in the available literature. They are likely reduced function variants but the degree of reduced function is not certain.
Gene by Gene Approach – NQO1 +/-
NQO1, which is induced by Nrf-2, reduces (reverses oxidation) procarcinogenic quinones (molecules where a hydroxy (-OH) group has been oxidized). This is a null mutation, such that NQO1 activity is not present. Our approach here is to optimize your antioxidant defenses and remove from your physiology pro-oxidant metals and organic pollutants.
Plan of Action – SOD2 +/+, CAT +/+, and NQO1 +/-
1. If we identify oxidative stress
on your NutrEval than GliSODin 250 mg/day and 1-2 Glutaclear/day would make
sense.
2. Grounding (otherwise known as “Earthing”) provides an antioxidant effect. My
colleague Dr. Steve Sinatra wrote a book on this issue and you can obtain
grounding pads from his website (cost is relatively low).
Detoxification Genes
Gene by Gene Approach CYP2D6 rs1135840
CYP2D6 metabolizes a large number of prescription drugs (please
see list in attached table), such that greater than usual doses might be
required. This SNIP is felt to represent a normal or “wild type” enzyme. This
is probably not an issue for you as you are +/- for this SNIP.
Gene by Gene Approach – NAT2 +/- Up and Down Regulations
N-acetyltransferase 2 (NAT2) is involved in the activation and inactivation of numerous toxins (heterocyclic aromatic amines, hydrazine drugs, and carcinogens). Polymorphisms in this gene lead to rapid, intermediate, and slow acetylation phenotypes. Slow acetylators clear toxins slowly, associated with increased risk of malignancy, especially bladder, but also lung, colon, breast, and head and neck. Conversely, rapid acetylation status may increase risk of other malignancies, as acetylation may activate other pro-carcinogens. You are +/- for both fast and slow variant forms of NAT2. To address acetylation alleles and this metabolic step in general, please avoid smoke and charred meats, and emphasize fruits and cruciferous vegetables in your diet. Optimizing one’s nutritional status makes sense, and if cysteine is low, then N-acetyl cysteine supplementation would be in order.
Gene by Gene Approach – CYP2C19 rs12248560 +/-
CYP2C19 metabolizes a number of prescription drugs. The rs12248560 variant codes for an enzyme with increased functional activity. Thus you might need greater than usual doses of agent metabolized through the CYP2C19 pathway, such as PPIs (proton pump inhibitors), Citalopram, Escitalopram, diazepam, imipramine, and clomipramine. Conversely, this enzyme activates the anti-platelet agent Plavix, enhancing its biological effect.
Neurotransmitter Metabolism
Gene by Gene Approach and Plan of action - GCH1 +/+
GCH1 (GTP cyclohydrolase catalyzes the rate limiting step in BH4 generation. Being +/+ for this gene, your ability to generate BH4 may be impaired. Oxidative stress leads to BH4 insufficiency while resolving oxidative stress will increase BH4 activity. BH4 and higher dose methyl folate supplementation can be used if we feel that BH4 physiology is suboptimal. Methyl-folate is to be initiated at a dose of 400 mcg/day. In the future BH4 at a dose of 2.5 mg/day will likely be added.
Gene by Gene Approach – Tyrosine Hydroxylase +/+
Tyrosine Hydroxylase generated dopamine from tyrosine. TH rs6356 codes for reduced function of this enzyme. Thus dopamine production will be compromised. Dopamine production can be increased with precursor (tyrosine, N-acetyl-tyrosine, or macuna purines) supplementation (you have tyrosine on board now), Vitamin D supplementation, and by ensuring that BH4 and SAMe co-factors are available. Dopamine breakdown by COMT and MAO can be blunted by quercetin and turmeric. Reduced BH4 availability due to +/+ status for GCH1 (generates BH4) and DHFR +/- (recycles BH4) could also compromise dopamine generation.
Gene by Gene Approach – MAO A +/+ for Loss of Function Allele
MAO A breaks down serotonin and to a lesser extent dopamine and norepinephrine. When COMT is dysfunctional (either on a genomic basis or due to a low SAMe:SAH due to elevated homocysteine or SAH), MAO A picks up some of the slack. MAO A is stimulated by progesterone and inhibited by Curcumin (turmeric). MAO A reduced function may be associated with an increased tendency to mood swings and panic disorders, related to fluctuations in serotonin levels. Serotonin formation may pick up as BH4 levels are restored with other maneuvers to address methyl cycle abnormalities. Tryptophan in food is converted into serotonin and tyrosine in food in to dopamine. If one is abnormal for a MAO A down regulation and normal for COMT, then emphasizing foods higher in tyrosine than in tryptophan makes sense. NutrEval testing will give us 5-HIAA, the breakdown product of serotonin metabolism, and should shed light on this issue. Sanesco testing will also help us optimize your serotonin status.
Toxin Susceptibility
Gene by Gene Approach - BDNF +/+
NTRK2 (and here you are genomically normal) stimulates production of neuroprotective BDNF (Brain Derived Neuroprotective Factor), which is not working well in you as you are +/+ (abnormal function) for BDNF. Reduced BDNF activity is felt to render one more susceptible to adverse neurologic effects from toxins.
Plan of Action - BDNF +/+
Our plan here will be to remove all toxic molecules form your body. Did your biological Mother bear amalgam fillings? Did she smoke or was she exposed to second hand smoke (tobacco is a source of cadmium which readily crosses the placenta.
Estrogen Metabolism
Gene by Gene Approach - CYP1A2 +/- Reduced Function
CYP1A2 is involved in Phase I (activation) detoxification. CYP1A2 thus activates a fat soluble toxin, such that it can be bound to a chaperone molecule (such as glycine or taurine or a methyl group) by a Phase II enzyme. CYP1A2 also carries out 2-hydroxylation of estrogen molecules, rendering them less active, and amenable to methylation by COMT to creat the cardioprotective and malignancy preventing 2-methoxyestrogen molecules. CYP1A2 is specifically involved in caffeine metabolism. Caffeine leads to the release of stimulatory neurotransmitters such as dopamine and norepinephrine (making us feel alert). These neurotransmitters are broken down by COMT. Individuals who are + for CYP1A2 and + for COMT will be caffeine sensitive and are at greater risk for adverse cardiovascular effects with high coffee intake.
Gene by Gene Approach CYP1B1 +/+ Increased Function
CYP1B1 is involved in Phase I (activation) detoxification. CYP1B1 thus activates a fat soluble toxin, such that it can be bound to a chaperone molecule (such as glycine or taurine or a methyl group) by a Phase II enzyme. CYP1B1 also carries out 4-hydroxylation of estrogen molecules, rendering them more active, and susceptible to oxidation in to 4-quinones, which can damage our DNA and lead to increased risk of breast and prostate malignancy. Up regulated CYP1B1 activity not accompanied by appropriate Phase II detoxification (such as when glycine, taurine, and glutathione are in short supply or if COMT is dysfunctional) can lead to oxidative stress.
Plan of Action – CYP1A2 +/- and CYP1B1 +/+
Estrogen metabolism and risk of reproductive organ malignancy is not an issue for you. Supplements that increase Nrf-2 translocation will increase production of CYP1A2.
Gene by Gene Approach and Plan of Action – NOS3 +/+
NOS (Nitric Oxide Synthase) in a BH4 dependent reaction, converts Arginine in to Nitric Oxide, our most important vasoprotective molecule. NOS is also involved in ammonia detoxification. Our treatment here includes previously described efforts to lower your ammonia burden, in adults our general cardiovascular treatments designed to improved endothelial function (which is dependent on nitric oxide) and the addition of BH4 to your program after urine sulfate levels have fallen. We can measure endothelial function in the office with EndoPAT testing (likely available close to home – not an issue at your age).
Gene by Gene Approach – Methyl Thieves and SAMe Stealers
A key goal of Methyl Cycle physiology (and a focus in our work with you) is to
ensure sufficient, replenishable, and physiologic (not excessive) supplies of:
A. SAMe, along with and an appropriate SAMe to SAH ratio (it is the ratio, not
just the SAMe level, that drives forward useful methylation reactions).
B. BH4 (needed to generate neurotransmitters and nitric oxide), and
C. Key antioxidant and detoxification molecules (glutathione, taurine, sulfate,
and cysteine).
D. Purine and Pyrimidine bases for DNA and RNA generation.
You are generating (or taking) methyl folate and methyl B12, not for the sake of
generating high levels of these Methyl Cycle intermediates (yes, intermediates,
not finished products), but rather to help ensure that the Methyl Cycle work
products (SAMe, BH4, glutathione, cysteine, and taurine) are in adequate supply.
While our focus has been on improving SAMe supply, we should also consider means
to reduce SAMe expenditure (Mother Nature balances supply and demand – the
government should pay heed)! Stated otherwise, if nutritional supplementation
decreases demand for SAMe, more will be available to meet critical demands (e.g.
DNA methylation to silence inflammatory and proto-oncogenes).
So how are we “spending” SAMe? What phenomena lead to SAMe wasting or
diversion? How do we ameliorate these pathophysiologies to restore SAMe and
appropriate SAMe:SAH balance?
In considering SAMe expenditure, remember that each time we
“spend” a SAMe (S-Adenosylmethionine) to carry out a specific methylation
reaction, we create a SAH
(S-Adenosylhomocysteine), which in turn inhibits methylation. A declining
SAMe:SAH inhibits methylation reactions; it does us no good to increase SAMe if
at the same time we buildup SAH.
Fortunately, SAH is rapidly converted to Homocysteine and Adenosine (except in you, where your AHCY +/+ status may compromise conversion of SAH in to homocysteine). Adenosine is efficiently removed, but if the Methyl Cycle is sluggish, due either to SNIPS, toxins, or nutritional deficiency, Homocysteine will build up. Homocysteine will then be back converted to SAH, the SAMe:SAH ratio falls, and useful methylation grinds to a halt. Homocysteine itself is not the problem; it is the buildup of SAH, compromising methylation potential, which leads to disease states such as atherosclerosis, cancer, and mood disorders.
So what processes “steal” SAMe? In considering this issue,
we need to be aware that CBS (which irreversible drains Homocysteine down the
trans-sulfuration pathway and away from SAMe reformation) is up regulated
(enzymatic activity increases) by oxidative stress and inflammation.
A. Oxidative stress:
When the generation of free radicals (superoxide, hydroxyl, and hydrogen
peroxide) outpaces our ability to neutralize them with endogenous (e.g.
superoxide dismutase) or exogenous (supplemental antioxidants), we suffers from
a buildup of free radicals. To address this immediate threat to health,
Homocysteine metabolism down the CBS pathway (irrespective of SNIP status) will
increase. Homocysteine (and with it the potential to create new SAMe) will be
irreversibly diverted away from remethylation (via MTR and BHMT back into
methionine for conversion to SAMe) and towards the production of glutathione,
taurine, and cysteine.
This all makes sense. Oxidative stress damages our physiology and kills cells. When faced with oxidative death, it makes sense to divert Methyl Cycle resources towards antioxidant generation. After oxidative stress has been neutralized, CBS flow will decrease, Homocysteine will start flowing back towards SAMe, and useful methylation reactions will resume. Our problem is that most ill Americans suffer from unremitting oxidative stress (we can measure your individual level of oxidative stress with the NutrEval study). Homocysteine will thus be shunted down the CBS pathway, such that useful methylation of DNA, estrogen molecules, and catecholamines will be compromised. If you cannot methylate catecholamines, then oxidative stress will develop within your blood vessels. If you cannot methylate your DNA, than you cannot silence inflammatory genes. You thus make more inflammatory molecules, more free radicals build up, more Homocysteine is diverted away from SAMe regeneration, and you are now chronically ill.
The solution is to undergo an assessment of oxidative stress, and then takes steps to resolve any challenges present. This will involve removing from your body phenomena that generate free radicals (e.g. smoking, toxic metals, organic pollutants) while concomitantly shoring up your antioxidant defenses with nutrients that we find to be in short supply (selenium, Vitamin E, Vitamin C, etc.). We can thus use nutritional medicine to help you generate SAME and to prevent oxidative stress from “stealing” Homocysteine away from SAMe regeneration. As a side note, toxic metals not only “steal” SAMe, they also compromise its formation (e.g. Mercury compromises MTR, in this fashion blocking useful remethylation of Homocysteine back into methionine for conversion into SAMe). Your genomic antioxidant reduced function genes (SOD2, CAT, and NQO1) predispose you to oxidative stress. Reduced ability to clear free radical generating toxins, due to your glutathione down regulations may also lead to oxidative stress.
B. Inflammation: Inflammatory TH1/TH17 cytokines, such as TNF-alpha, Il-6, and Il-1b also increase flow down the CBS pathway, draining Homocysteine away from useful remethylation back in to SAMe. Inflammation leads to oxidative stress and oxidative stress leads to inflammation. Both are useful in fighting infection, but both processes are persistently elevated as our immune system misinterprets as infection the chronic “pseudoinfections” of visceral obesity, leaky gut, and environmental toxicity. Thus by resolving inflammation (either with anti-inflammatory nutrition interventions such as turmeric or berberine) or by removing the cause of chronic inflammation (weight loss or resolving leaky gut) we can resolve the “inflammatory drain” on SAMe supply and demand.
You harbor (or did harbor) several infections and this
will cause chronic inflammatory stress. A new approach is the use of Resolvins,
fish oil downstream metabolites that tell the immune system to switch from
inflammation to inflammation resolution. The preparation is Metagenics
OmegaGenics SPM Active. Given your size one daily should help with inflammation
reduction (you can order this from the Metagenics website – heartfixer.com
provides a link). Resolvin therapy will not prevent you from mounting an
appropriate response to infection, but it will help reduce inappropriate chronic
inflammation.
What processes deplete our SAMe stores? Are some less critical than others?
Can we decrease SAMe demand with nutritional supplementation?
A. DNA methylation: This is sacrosanct. Only SAMe can methylate DNA. Only SAMe can shut down the transcription (reading into protein formation) of viral, inflammatory, and proto-oncogenes (promote cancerous transformation) while maintaining the transcription of tumor suppressing and anti-inflammatory genes. We can’t scrimp on DNA methylation, but by resolving oxidative/inflammatory stress, and supplementing with SAMe “sparers” as described below, we can maintain adequate SAMe (with a high SAMe:SAH ratio) to ensure optimal DNA methylation.
B. Creatine formation: Around 50% of our SAMe is “spent” in the generation of creatine, a molecule critical to energy maintenance. We do work by splitting a high energy bond within ATP (Adenosine Triphosphate) to produce ADP and phosphate. We burn carbon and use this energy to rephosphorylate ATP. When energy is plentiful, ATP will transfer a phosphorus group to creatine, forming Phosphocreatine. Should we suddenly run out of ATP energy (sprinting, weight lifting, or if oxygen supply:demand is compromised by a blocked artery or failing heart), Phosphocreatine can download a high energy phosphate bond back to ADP, regenerating ATP such that cellular work can continue. We actually store 10 heart beats of energy as Phosphocreatine. As you would expect, creatine supplementation has been shown to be helpful in anaerobic athletic performance as well as in heart failure. Of interest, creatine has been shown to lower cholesterol, and while the literature is not 100% consistent, creatine supplementation will decrease expenditure of SAMe and increase the SAMe:SAH ratio. Creatine lowers homocysteine in individuals with MTHFR abnormalities. Athletes take 5 grams of creatine, four times a day (saturation dose) for one week, followed by 5 grams/day (maintenance dose). However, unless you have an athletic competition coming up, you can simply add 5 grams of creatine/day to your program. Creatine is not unsafe, but there have been instances where competitive body builders dosed up on creatine while decreasing fluid intake (so their muscles will bulge out more) leading to dehydration and kidney compromise. Creatine is converted in to Creatinine, which is filtered out by the kidneys. We use serum creatinine to gauge kidney function. A trivial rise in serum creatine may occur when you supplement with creatine. This does not mean that kidney function is decreasing; rather this is an artifact due to creatine supplementation. Creatine supplementation at 5 grams/day makes sense for individuals with Methyl Cycle SNIPS that might compromise SAMe generation or maintenance (MTHFR, MTR, and BHMT), or when we feel that chronic oxidative/inflammatory stress is depleting SAMe regeneration.
C. Phosphatidylcholine: Three SAMe molecules, around 30% of our total supply, are used to methylate phosphoethanolamine into phosphatidylcholine. Phosphatidylcholine (PC) is involved in lipoprotein formation and reverse cholesterol transport; PC is also a critical component of the cell membrane. The common name for PC is lecithin. PC/lecithin is essentially a triglyceride like molecule with two fatty acids and one phosphocholine group attached to a three carbon glycerol backbone. The biochemical utility of PC relates to the composition of its two fatty acids. PC containing two unsaturated linoleic acid molecules (polyenylphosphatidylcholine) is used IV and orally to treat cardiovascular, liver, and neurological disease (see our DVD presentation). If we supplement you with PC, less SAMe will be spent generating PC, and more will be available for useful methylation reactions. In addition, the less SAMe spent, the less SAH and Homocysteine will be formed. Furthermore, PC can be converted into choline, which can be converted into Betaine (TMG or trimethylglycine) which is used by BHMT to directly remethylated homocysteine back in to methionine (which is then converted in to SAMe). Thus PC supplementation will lower an elevated Homocysteine and increase SAMe supply along with the SAMe:SAH ratio. We use PhosChol (unsaturated phosphatidylcholine rich in linoleic acid) 900 to 2700 mg/day in the treatment of cardiovascular and liver disease. Our dose in Methyl Cycle patients will relate to your SNIP status and baseline Homocysteine level. Your +/+ status for PEMT compromises phosphatidylcholine generation and thus PC support will be important.
D. COMT utilization. COMT (Catechol-O-Methyl transferase) metabolizes estrogen molecules, catecholamines (dopamine and norepinephrine), drugs (e.g. L-Dopa used in the treatment of Parkinson’s disease) and bioflavonoids (particularly Quercetin) by transferring a methyl group from SAMe to an oxygen molecule on the compound being methylated. Each time this occurs, SAH is generated, the SAMe:SAH ratio falls, and COMT and all other methyl-transferase enzymes are inhibited. If we are interested in sparing SAMe and maintaining a high SAMe;SAH ratio, it would be prudent to reduce the need for COMT-driven methylation. Lowering stress will lower norepinephrine, and thus decrease SAMe utilization by COMT. While bioflavonoids such as Quercetin have many beneficial properties, if SAMe preservation is critical (high Homocysteine in the presence of MTHFR, MTR, MTRR, and BHMT SNIPs or if our ability to methylate estrogen molecules is impaired) then decreasing intake of Quercetin and related bioflavonoids would be prudent. Conversely, when insufficient dopamine is the problem, we might use Quercetin to blunt dopamine degradation by “clogging up” COMT. Caffeine increases catecholamine production. Caffeine intolerant individuals are typically COMT +. When caffeine intolerance develops anew, we look for new problems that might be compromising SAMe supply or COMT functionality.
Plan of Action for Methyl Thieves and SAMe Stealers )
1. NutrEval assessment will give us information as to the level of
oxidative and inflammatory stress that you are experiencing.
2. Phosphatidylcholine is already present in your program; if SAMe is low we may
wish to increase the dose.
3. Creatine 5 grams/day (mixed in a liquid) to spare SAMe may be added in the
future (if further testing or your clinical response suggests that SAMe is low
or that your SAMe:SAH ratio is low).
4. Metagenics OmegaGenics SPM Active one daily makes sense.
Additional Thoughts
Thank you for your patience with respect to the time required to construct your report. It takes me considerable time to analyze the data and construct the reports, and I have been busy this summer creating several new physician presentations for upcoming medical meetings.
Your genomic predispositions are likely playing an important role in your health, particularly with respect to impaired clearance and sensitivity to environmental toxins. Individuals with your genomic pattern existed 50 years ago but Autism and related neurodevelopmental conditions did not exist until we introduced these metals and organic pollutants in to the environment - so we need to remove these molecules from you.
Please share all of this information with your other health care providers. They know your situation far better than I do at this point.
This report may contain typos. If you see a typo let us know and I can correct it.
I did put more energy than usual in to your report. Others might benefit from this information. If OK with yourself I would like to post your report (anonymously of course) on the heartfixer.com website. If OK with yourself please send back a copy of your signed OK.
After you have had a chance to review this report we can have an initial (no charge to compensate your for the long delay) 30 minute phone conference to map out your initial testing and treatment strategy. If you wish to come to Toledo for MME please contact Debbie Braun, our practice manager.
James C. Roberts MD FACC FAARFM 10/11/15
Sample Report - Adult with Chemical Sensitivity
|
Methyl Cycle Nutrigenomic Report for Adult with Chemical Sensitivity |
||
|
Methylation Panel Abnormalities for Genes with Characterized SNPs |
||
|
Gene Name |
Variation |
Finding |
|
COMT |
V158M |
OK |
|
COMT |
H62H |
OK |
|
COMT |
P199P |
OK |
|
VDR |
Taq |
Homozygous (+/+) |
|
VDR |
Bsm |
OK |
|
MAO A |
R297R |
Heterozygous (+/-) |
|
ACAT |
102 |
OK |
|
MTHFR |
C677T |
Heterozygous (+/-) |
|
MTHFR |
3 |
Heterozygous (+/-) |
|
MTHFR |
A1298C |
Heterozygous (+/-) |
|
MTR |
A2756G |
OK |
|
MTRR |
A66G |
Heterozygous (+/-) |
|
MTRR |
H595Y |
Heterozygous (+/-) |
|
MTRR |
K350A |
Heterozygous (+/-) |
|
MTRR |
R415T |
OK |
|
MTRR |
A664A |
OK |
|
BHMT |
2 |
Homozygous (+/+) |
|
BHMT |
4 |
Homozygous (+/+) |
|
BHMT |
8 |
Homozygous (+/+) |
|
AHCY |
1 |
OK |
|
AHCY |
2 |
OK |
|
AHCY |
19 |
OK |
|
CBS |
C699T |
Homozygous (+/+) |
|
CBS |
A360A |
Heterozygous (+/-) |
|
CBS |
N212N |
OK |
|
SHMT |
C1420T |
Heterozygous (+/-) |
|
CYP2D6 |
rs16947 2850C®T |
Homozygous (+/+) |
|
ACE Del16 |
|
Heterozygous (+/-) |
|
MTHFD1 |
rs2236225 |
Homozygous (+/+) |
|
DHFR |
rs1643649 |
Heterozygous (+/-) |
|
SLC19A1 |
rs3788200 |
Heterozygous (+/-) |
|
PEMT |
rs7946 |
Homozygous (+/+) |
|
GAD1 |
rs3749034 |
Homozygous (+/+) |
|
CYP1A1 |
rs2606345 |
Homozygous (+/+) |
|
CYP1A2 |
rs72547513 |
Homozygous (+/+) |
|
CPOX4 |
rs1131857 |
Heterozygous (+/-) |
|
BDNP |
rs6265 |
Heterozygous (+/-) |
|
NTRK2 |
ss2769605 |
Homozygous (+/+) |
|
SOD2 |
A16V rs4880 |
Homozygous (+/+) |
|
SOD3 |
C498T rs2855262 |
Homozygous (+/+) |
|
GSTP1 |
rs1695 |
Heterozygous (+/-) |
|
NAT2 |
rs1208 |
Homozygous (+/+) |
|
NAT2 |
rs1801280 |
Homozygous (+/+) |
|
NR3C1 |
|
Heterozygous (+/-) |
|
NOS3 |
rs2070744 T786C |
Homozygous (+/+) |
|
ADIPQ |
rs1501299 and rs3774261 |
Heterozygous (+/-) |
Overview
The function
of the Methyl Cycle is to maintain (current health status) appropriate levels
of:
A. SAMe, along with a high SAMe:SAH ratio, necessary for biological methylation.
B. BH4, need to generate neurotransmitters and nitric oxide.
C. The antioxidant/detoxification molecules cysteine, taurine, sulfate, and
glutathione.
D. Purine and Pyrimidine bases for DNA and RNA generation.
You are homozygous (+/+) for the CBS C699T and heterozygous (+/-) for the A360A up regulations and homozygous (+/+) for all three BHMT down regulations (which behave like CBS up regulations). Homocysteine (and its Methyl Cycle precursors) is thus being drawn down the trans-sulfuration pathway, in this process generating excessive sulfur break down products (sulfite and sulfate, which stimulate the stress/cortisol “fight or flight” response), too much excitotoxic glutamate (which you are having some trouble converting in to GABA due to your GAD1 +/+ status), and too much ammonia (which depletes BH4, contributing to insufficient dopamine and serotonin production), and too much hydrogen sulfide (which produces brain fog).
This deficiency in BH4 predisposes NOS3 (endothelial nitric oxide synthase) to convert Arginine in to free radicals as opposed to nitric oxide, predisposing you to oxidative stress and future hypertension and cardiovascular disease. Compounding this problem you are +/+ for NOS3, compromising your ability to generate nitric oxide and metabolize ammonia, and +/- for ACE, which tends to increase production of the vasoconstricting and pro-oxidant angiotensin II. Your DHFR (+/-) status (and possibly your MTHFR A1298C +/- status) may also compromise BH4 recycling, so with respect to the precious molecule BH4, you are getting hit at both ends – reduced recycling and increased utilization. After the problems in the trans-sulfuration pathway (CBS and BHMT) have come under control, BH4 or additional methyl-folate as a BH4 precursor/mimic can be added to your program.
In dealing with oxidative stress you are challenged by +/+ status for SOD2 (mitochondrial superoxide dismutase) which neutralizes mitochondrial superoxide and +/+ status for SOD3 (extracellular superoxide dismutase) which protects the endothelial vascular lining and the nitric oxide synthase enzyme itself from the damaging effects of free radical superoxide.
Folate
molecules serve to transfer methyl groups within our physiology (think of
folates as “methyl group taxis”). To become useful, the oxidized dietary folate
molecules that we take in must first be reduced to Tetrahydrofolate (THF) by
dihydrofolate reductase (DHFR). You are (+/-) for a DHFR reduced function
allele, such that conversion of dietary folates in to useful THF may be
compromised. SHMT (serine hydroxyl methyl transferase; your genomic status is
+/-), a pyridoxal-5-phosphate dependent enzyme, tacks on a methyl group derived
from the amino acid serine to generate 5,10-MethyleneTHF, which is then
converted to 5-methyl folate by MTHFR.
5,10-MethyleneTHF can also be acted upon by MTHFD1,to generate the building
blocks for DNA and RNA generation. Being +/- for MTHFD1, you may be having
trouble with these steps and in recycling folates back into THF. SLC19A1 +/-
status compromises folate transport across the cell membrane. We can address
these alleles with a balanced regimen involving folinic acid, folate, and
methyl-folate supplementation.
CBS actually generates sulfite, which is converted in to less toxic sulfate by SUOX, an enzyme that becomes “overworked” and “co-factor depleted”. We can support SUOX function by supplementing you with its co-factors molybdenum, boron, Vitamin E succinate, and hydroxy-B12.
The high levels of sulfur break down products may (Dr. Yasko’s position) compromise the absorption of detoxifying sulfur based molecules (cysteine and glutathione) in to your cells, compromising endogenous detoxification (setting you up for organic pollutant and heavy metal overload). In addition, your COPX4 +/- status places you at increased risk for biochemical damage due to mercury exposure (BDNP +/-, NTRK2 +/+, and GSTP1 +/- status may also play a role in increased susceptibility to mercury). You bear +/+ SNIPS for both gain of function and reduced function with respect to detoxification involving acetylation. GSTP1 +/- status compromises your ability to utilize glutathione in the detoxification process. CYP1A1 and 1A2 +/+ status compromises your ability to initiate phase I detoxification of hydrocarbon toxins. We will address these genomic predispositions to impaired detoxification with nutritional support of the detoxification process and specific detox strategies based upon your individual toxin burden.
MTR uses 5-methyl folate and methyl-B12 to convert homocysteine in to methionine, which is then converted by methionine adenosyltransferase (MAT) in to SAMe, the universal methyl donor. You are +/- for several hepatic (MAT1) alleles and +/+ for several extra hepatic (MAT2) alleles (the literature is not clear here but these MAT SNIPs are probably not functionally significant). You are +/- for at least two of the MTRR alleles, meaning that you are having trouble converting B12 in to methyl-B12, a problem that can be addressed with methyl-B12 supplementation. You are +/+ for VDR Taq, such that Vitamin D will be less efficient in generating dopamine, and -/- for COMT, meaning that you can breakdown dopamine rapidly, using up methyl groups in doing so, and thus you will have an increased susceptibility to toxic metals and viral infection. Conversely, your need and tolerance for methyl groups and methyl donors will be relatively increased (any symptoms that you might experience with methyl donors will not reflect sensitivity to methyl groups but rather sensitivity to sulfites/ammonia/glutamate that are generated when these agents spin forward the Methyl Cycle and homocysteine is drawn down the up regulated CBS “drain”).
You are +/-
for MTHFR C677T and MTHFR 3, meaning that you are having some trouble converting
folic acid(or more specifically 5,10-Methylene THF) in to 5-methyl folate, a
strain that is easy to overcome with either (or both) 5-methyl folate or
riboflavin supplementation.
+/- status for MTHFR A1298C also compromises methyl-folate generation. Dr. Yasko
(other authors do not agree with this position) feels that this SNIP also blunts
recycling of spent BH2 back in to BH4.
Folate molecules serve to transfer methyl groups within our physiology (think of folates as “methyl group taxis”). To become useful, the oxidized dietary folate molecules that we take in are first reduced to Tetrahydrofolate (THF) by dihydrofolate reductase (DHFR). Being +/- for DHFR, half of your DHFR molecules are not functioning optimally. Your +/- status for FOLR1 and FOLR2 and +/+ status for SCL19A1 compromise transport of folate molecules within your physiology and thus you may need great levels of folate molecules than individuals who are wild type (-/-) for these genes.
SHMT (serine
hydroxyl methyl transferase – your genomic status is +/-), a
pyridoxal-5-phosphate dependent enzyme, tacks on a methyl group derived from the
amino acid serine to . generate 5,10-MethyleneTHF, which is then converted to
5-methyl folate by MTHFR.
5,10-MethyleneTHF can also be acted upon by MTHFD1,to generate the building
blocks for DNA and RNA generation. Being +/- for MTHFD1, you may be having
trouble with these steps and in recycling folates back into THF. Being +/+ for
MTHFS, you are having some trouble breaking down folinic acid. We can measure
folate metabolites, and supplement you based upon the results, or we could use a
combination of low dose folinic acid along with methyl-folate.
PEMT (which is stimulated by estradiol) uses three SAMe molecules to generate phosphatidylcholine. You are +/+ for a loss of function PEMT allele, and thus you are having trouble generating phosphatidylcholine. We use phosphatidylcholine in the remethylation of homocysteine into methionine by BHMT (also pulling homocysteine away from the “CBS drain”), in lipid metabolism, and in the generation of the neurotransmitter acetylcholine. Phosphatidylcholine supplementation makes sense here. We spend 2/3rds of our SAMe in the generation of phosphatidylcholine and creatine, and supplementation with these substances will spare SAMe for other more critical activities (such as maintaining proper DNA methylation and in the generation and break down of neurotransmitter substances).
You are +/+ for VDR Taq, such that Vitamin D will be less efficient in generating dopamine, and -/- for COMT, meaning that you can breakdown dopamine rapidly, using up methyl groups in doing so, and thus you will have an increased susceptibility to toxic metals and viral infection. Conversely, your need and tolerance for methyl groups and methyl donors will be relatively increased.
Being +/- for MAO A, you are having some trouble breaking down serotonin, an issue that we can address by favoring foods rich in tyrosine, the precursor to dopamine, which you need, over foods rich in tryptophan, the precursor for serotonin.
Caffeine leads to release of cortisol and catecholamines (epinephrine and norepinephrine) from the adrenal glands. If your SAMe:SAH ration is favorable, being -/- for COMT you will be able to break these molecules down via methylation. However, being +/+ for CYP1A2, you are having trouble metabolizing caffeine, and this may render you caffeine sensitive. Being+/- for NR3C1, your cellular responsiveness to cortisol may be compromised, and this may set you up for cortisol excess and weight gain. Being +/- for ADIPQ, production of the anti-atherosclerotic, anti-obesity adipokine adiponectin is compromised. CYP2D6 C2850T +/+ status is associated with overly rapid metabolism of several prescription drugs, such that you might need greater than usual doses is one of these agents is appropriate for a specific health challenge.
You are +/- for one of the GAD (involved in interconversion of glutamate into GABA) impaired function alleles, setting you up for glutaminergic excitotoxicity, which we can address with
Your genomic findings are significant. They place you at risk for environmental toxicity and oxidative stress, both of which lead to inflammatory stress and auto-immunity. Our initial plan will be to evaluate and mitigate the effects of your up regulated homocysteine trans-sulfuration status (CBS and BHMT) as we evaluate your nutritional status and rectify any deficiencies present. Then we will take aim at optimizing SAMe generation and utilization, and then take aim at your toxic burden.
The Gene by Gene sections provide generic information while recommendations for your genomic pattern are described in the Plan of Action sections. As stated above, we need to keep in mind that while your genotype (discussed here) may impact your health, your phenotype (how these genes effect your physiology – your overall health status) is determined by other phenomena, such as diet, environmental toxin exposure, and life style. Thus each and every recommendation I make may not be appropriate for you. We also need to ensure that these recommendations do not conflict with the care that you are receiving from your other practitioners. Based upon review of your medical history and genomic status I have a few ideas as to further analysis and treatment. Approaches that make the most sense to me receive a (Ö). Those that are less critical (or more costly) are designated (+/-). We can certainly discuss all of this.
Gene by Gene Approach – CBS +/+ and +/- with BHMT +/+
CBS
(Cystathionine Beta-Synthase) is discussed on pages 48-53 of Dr. Yasko’s book,
Genetic Bypass. You are +/+ (all of your CBS enzymes are abnormal) for the CBS
C699T and +/- (half of your CBS enzymes are abnormal) for the CBS A360A up
regulations and +/+ (all of your CBS enzymes are abnormal) for all three of the
major BHMT down regulations (which act like CBS up regulations). Homocysteine
(and its Methyl Cycle precursors) is being drawn down the trans-sulfuration
pathway, in this process generating excessive sulfur break down products
(sulfite and sulfate, which stimulate the stress/cortisol “fight or flight”
response – although your sulfate levels have not been elevated), too much
glutamate (which leads to glutaminergic excitotoxicity – a double problem for
you as your GAD +/- status compromises interconversion of glutamate and GABA),
hydrogen sulfide (to produce brain fog), and too much ammonia (which depletes
BH4, leading to insufficient serotonin and dopamine production. A deficiency in
BH4 allows NOS (nitric oxide synthase, which is not working optimally in you as
you are +/+ for NOS3) to convert arginine in to free radicals as opposed to
nitric oxide, predisposing you to hypertension and cardiovascular disease.
Being +/- for DHFR, you are having trouble regenerating BH4, so with respect to
the precious molecule BH4, you are getting hit at both ends – reduced production
and increased utilization. Thus your ability to generate neurotransmitters and
nitric oxide will be compromised. Instead your genomic status predisposes
nitric oxide synthase to generate the free radicals superoxide and
peroxynitrite, which lead to oxidative stress and inflammation. Compounding
this predisposition towards increased production of superoxide, your +/+ status
for SOD2 (mitochondrial) and SOD3 (extracellular) compromises your ability to
neutralize superoxide.
I realize that this sounds awful but these are all issues that we can deal with, now that we understand their origin and biological significance.
During normal physiology, metabolic flow down the CBS pathway is designed to generate the important anti-oxidant and detoxifying molecules glutathione, taurine, cysteine, and alpha-ketobutyrate (which Dr. Yasko feels can be converted into GABA, a calming neurotransmitter, or glutamate, an excitotoxin; others dispute this position but we typically see elevated glutamate in individuals with CBS/BHMT + alleles).
The CBS C677T and A360A genes code for enzyme function that is up regulated (faster than usual - your ancestors needed antioxidant support more than they needed methylation support; thus these SNIPs which direct homocysteine towards glutathione and away from SAMe regeneration). Of the two, the C677T allele is the most important, producing enzyme activity that is 10 fold greater than normal. You thus suffer from “too much of a good thing and way too much of several bad things”.
Oxidative stress (the accumulation of free radicals) increases flow down the CBS pathway, to generate the above listed antioxidants needed to allow the body to respond to an oxidative challenge – a good thing. However, when homocysteine is drawn down the CBS pathway, it is “lost forever” such that it cannot be remethylated and used to regenerate SAMe. In this fashion oxidative stress (something we wish to avoid) leads to reduced SAMe (stated otherwise, your low reduced glutathione and Vitamin C status will pull homocysteine down the CBS pathway and away from SAMe regeneration). SAMe itself stimulates flow down the CBS pathway (if you have plenty of SAMe you do not need to worry about recycling it); this is why we advise you not to begin SAMe (or push with measures designed to up regulate SAMe production) until your CBS/BHMT alleles have come under metabolic control.
SAMe has been used to treat lead overload (and presumably will work against mercury), as SAMe stimulates CBS, which inevitably converts homocysteine into glutathione. Thus if you feel poorly with Methyl Cycle supplements, it may be due to a “detox reaction” (or it may be due to increased production of sulfite/sulfate, ammonia, and hydrogen sulfide).
While sulfate and sulfhydryl (-SH) bearing molecules are important in detoxification, sulfate/sulfite/-SH excess seems to block cellular up take of the key detoxifiers glutathione and cysteine (this is Dr. Yasko’s position; I can’t back this up from my review of the scientific literature but her position seems to work in practice). Endogenous detoxification is thus blunted (nearly all kids with Autism Spectrum Disorders bear CBS up regulations – why they are compromised by environmental toxins and the kid next door is just fine – could this be playing a role in your otherwise difficult to explain health conditions)? Conversely, after we decrease your sulfate/sulfite pool, your detox pathways will open up (and why, if we move too fast, you will experience detox phenomena).
The excess ammonia generated (you note an ammonia odor when you sweat) must be detoxified, and to do so BH4 (tetrahydrobiopterin) must be “spent” (far infrared sauna promotes detox and increases BH4). This is a problem in that we need BH4 to generate neurotransmitters (serotonin to maintain calm/prevent depression and dopamine to maintain motivation and drive). Without BH4, we cannot convert arginine in to nitric oxide; instead vascular wall toxic free radicals such as superoxide and peroxynitrite are created, leading to hypertension and cardiovascular disease.
Ammonia is metabolized within the urea cycle, an enzyme pathway that utilizes several amino acids (ornithine, aspartate, arginine, and indirectly alpha-ketoglutarate) to break down ammonia. Systemic ammonia detoxification takes place in the liver, and thus individuals with advanced liver disease experience hyperammoniaemia, with attendant neurological dysfunction (tremor, confusion, impaired coordination). We can thus borrow from the gastroenterology community in our approach to the hyperammoniaemia present in our patients with CBS/BHMT/MTHFR alleles (also giving me a chance to consult with our daughter, who is a gastroenterology fellow).
Intestinal microbes generate ammonia. Gastroenterologists use antibiotic therapy (Rifaxamin, a poorly absorbed antibiotic that does not enter the circulation) to sterilize the gut, thus blunting ammonia production. While we may recommend antimicrobial therapy if bacterial overgrowth is demonstrated on a CDSA (Comprehensive Digestive Stool Analysis), a basic approach will be to take a probiotic 2-3 times a day to promote a balanced intestinal flora (not a bad idea for all of us to deal with the effects of antibiotics found in grocery store meats).
Charcoal seems to absorb ammonia generated within the GI tract, and thus taking charcoal at bedtime seems to lower one’s ammonia burden (and you are utilizing charcoal as a detoxification aide). Charcoal can also cause constipation, a huge negative here, as moving your bowels 2-3 times a day is important in detoxification and ammonia neutralization. Thus we recommend charcoal three nights a week with magnesium citrate and/or Vitamin C as needed to promote normal GI tract motility (adjust doses to obtain a balance between ammonia neutralization and proper GI tract function – too much magnesium or vitamin C pulls water into the intestines, leading to loose stools and diarrhea). Gastroenterologists utilize the cathartic lactulose to accelerate GI tract motility, blocking ammonia absorption; we can achieve the same end nutritionally with vitamin C and magnesium.
Ornithine/Aspartate supplementation (LoLa), administered IV or orally, has been shown to be a safe and effective approach to ammonia reduction in liver failure, and we can utilize this low cost approach to deal with ammonia excess in Methyl Cycle patients, starting with 1000 mg (1/3rd teaspoon) three times a day, increasing to one teaspoon as needed. Aspartic acid has a glutamate-like stimulating effect, and if one experiences agitation/anxiety than aspartate can be dropped in favor of more ornithine. Ornithine monotherapy has been used to increase exercise capacity in healthy people, as ammonia production is a metabolic consequence of energy utilization. These and other amino acids are best absorbed on an empty stomach or with a carbohydrate; concomitant protein intake will blunt their absorption.
Dr. Yasko’s
diagrams indicate that CBS generates alpha-ketoglutarate, which can be converted
into glutamate. Actually, CBS generates alpha-ketobutyrate. Nonetheless,
individuals with CBS + alleles nearly always display elevated glutamate, and
thus the same physiology holds. We should be able to interconvert
alpha-ketoglutarate into glutamate, glutamine, and GABA. However, if glutamate
is in excess, or if toxic metals or GAD1 SNIPs (you are +/+ here)
compromise the interconversion enzymes, then we suffer a buildup of the
excitatory neurotransmitter glutamate. Glutamate is involved in alertness and
learning, but excess glutamate leads to irritability and over-excitement; toxic
levels may play a role in seizure activity and cardiac arrhythmia (could this be
why we are seeing so much more atrial fibrillation now then we were ten years
ago; MSG, a dietary source of glutamate, can precipitate atrial fib)?
CBS up regulations lead to an initial buildup of potentially neurotoxic sulfite,
which is then metabolized by SUOX (Sulfite Oxidase) to the less neurotoxic (but
still problematic at high levels) sulfate. SUOX activity requires molybdenum,
which is thus depleted in CBS + individuals. Homogenized dairy products contain
xanthine oxidase, which uses up molybdenum, and are best avoided or minimized.
Vitamin E succinate, boron, and B12 are felt to stimulate SUOX activity.
As methyl cycle function is needed in the biosynthesis of Co-Enzyme Q10 and Carnitine, individuals + for CBS will likely be energy depleted (and you noted improvement with CoQ10), and here supplementation (in relation to your COMT/VDR status) with Co-Enzyme Q10, Carnitine, Ribose, and NAD+ may be helpful.
BHMT (Betaine Homocysteine Methyl Transferase) directly methylates homocysteine back in to methionine, serving as a “back door” pathway to “pull” homocysteine away from the CBS “sulfate drain”. Thus if you bear CBS or BHMT abnormalities, it makes sense to support BHMT function. TMG (trimethylglycine) stimulates BHMT, and can be utilized if you are not overly sensitive to methyl group supplementation (based upon you COMT/VDR status). Phosphatidylserine stimulates BHMT (and we also use it to moderate elevated cortisol levels), as does phosphatidylcholine (which we use to treat vascular, liver, and neurologic disease states; your +/+ status for PEMT compromises phosphatidylcholine generation, particularly when estradiol is low) atherosclerosis. Phosphatidylcholine can be admixed with EDTA (detoxifies metals), creating a quite useful supplement.
Many of you with CBS and BHMT abnormalities will also bear MTHFR (compromising methyl-folate generation) and MTRR (compromising methyl-B12) abnormalities, and thus you will need and benefit from corresponding supplementation (with these molecules that they are having trouble making). However, if we treat you with methyl-folate, methy-B12, or BH4, before we have the CBS problem under control (sulfite/sulfate levels decreased enough to allow for appropriate glutathione and cysteine assimilation) then we will be subjecting you to “incomplete detoxification”. You will feel great for 1-2 days, as beneficial neurotransmitters are generated. Methyl-folate and methyl-B12 detox pathways will then open up, creating toxic intermediates that cannot be metabolized further due to the block in glutathione utilization – and you will feel horrible. Thus we need to resist the temptation to treat your MTHFR/MTRR abnormalities until CBS/BHMT are under control. You’ve lived your entire life with a gene set that is maladaptive to the toxic environment of modern man. It will take us some time to change your internal environment to “bypass” these genomic challenges.
Plan of action
for CBS +/- (BHMT discussed further in other sections)
To address this constellation of alleles I will recommend:
1. Moderate* animal protein
intake (anything with eyes) and avoid sulfur rich vegetables, sulfur containing
supplements, and sulfur containing drugs (see attached sulfur avoidance
instruction sheets and read Sulfites and Chronic Disease by Rick
Williams, available at the office or at www.readingtarget.com/nosulfites/.
2. Check the sulfate/sulfite content of your supplements and prescription agents
(many listed in the Williams book) and whenever possible switch to agents with
lower sulfate/sulfite content. Gelatin capsules may contain sulfate; thus if
possible switch to tablet or powdered forms of key supplements.
3. Monitor urine sulfate levels every 3-7 days (or when you feel particularly
good or poorly, or after adding a new treatment or changing your diet). Please
chart the levels – this will be our primary measuring stick – our goal is
a urine sulfate of 400 (one yellow and three pink) to 800 (two yellow and two
pink). Low levels will allow an increase in methyl cycle supplementation and
later the addition of BH4 and/or a liberalization of your diet. Conversely,
persistent high sulfate spills indicates that your diet/treatment program needs
further modification.
3. To neutralize ammonia (generated from animal protein), you can use Ammonia
Support RNA ½ dropper with meals and/or CBS RNA* (relatively expensive and thus
elective), along with a charcoal supplement at bedtime every other evening, away
from other supplements (magnesium citrate and Vitamin C may be used as needed to
keep the GI tract moving - optimally twice a day - as charcoal may lead to
constipation). Yucca, beginning at ½ capsule, twice a day, (or sprinkled on
food containing protein), may help with ammonia detoxification. A probiotic two
to three times a day makes sense. Ornithine/Aspartate 1000-3000 mg three times
a day (taken away from other sources of protein) will stimulate the urea cycle,
promoting ammonia degradation, and should increase your energy level. While
your ammonia level may not be elevated, BH4 is used up in ammonia metabolism, so
the less ammonia formed the better. We will measure your serum ammonia and
urine ammonia (GenovaLabs NutrEval study), so please do not start
Ornithine/Aspartate until the test samples have been obtained.
*Dr. Yasko’s CBS RNA product, to my understanding (which may be incorrect), is
an interference RNA, which blunts the production of CBS. I’m not exactly sure
of the biochemistry here and as these products are relatively expensive I do not
emphasize the RNAs, but you can try them and see if they help. You thus have
the option of adding her CBS Support as well as Ammonia Support RNA products to
your program (in theory this would allow you to take in more animal protein with
less homocysteine “spillage” down the CBS pathway).
5. Sparga Detox, 10 drops in water (wait at least one minute before consuming),
twice a day makes sense. Sparga was developed by fellow Cardiologist Dr. Lee
Cowden, specifically to address the CBS abnormality (see www.nutramedix.ec).
This is a less expensive approach to sulfite/sulfate neutralization.
6. To stimulate SUOX activity, we could add to your current program Boron 3 mg,
sublingual hydroxy-B12 2000 mcg/day, Vitamin E Succinate 400 IU daily, and
Molybdenum 150-500 mcg/day. (Designs for Health Complete Mineral Complex would
cover your need for Molybdenum and Boron). We will assess your mineral status
with a 24 hour urine for nutritional minerals and a serum iodine level.
7. Glutathione supplementation runs the risk of indirectly adding to your
sulfite/sulfate burden. Right now this “good thing” could actually set you
back. However, if we could convince your biochemistry to up regulate
biosynthesis of glutathione, then your anti-oxidant and detox capacity will
increase, with concomitant utilization of free sulfate/sulfhydryl groups – a
double win for you. This can be achieved with the use of the Life Wave
(needleless acupuncture) Glutathione patch. The Life Wave people have
demonstrated an increase in Glutathione levels in relation to patch use (please
see separate information sheet on Life Wave patch use). You are currently
receiving IV Glutathione, which we consider to be a powerful antioxidant and
detoxification agent, of definite value.
8. Your homocysteine and Vitamin D levels were checked recently and are within
the desirable range.
9. If you feel anxious or “wired up” (glutamate overload), take Zen (GABA 275 mg
plus Theanine, a methyl donor, 100 mg) twice a day. If this is helpful you can
double the dose. GABA does not work rapidly, but if you take it twice a day you
will build up a GABA reserve to balance any glutamate overload you might
experience. Magnesium supplementation may help with GABA physiology and often
helps with sleep.
8. You are already on Co-Enzyme Q. If energy (ATP) is low (and likely it is, as
otherwise you would not have noted such a positive response to Co-Q
supplementation) we could add to your program Carnitine 500 mg twice a day,
NAD+, and/or PQQ 10 mg twice a day. Ribose 5 gm two to three times a day may
also give you an energy lift; if so this would point to a problem in
mitochondrial ATP energy generation.
9. A Genova Labs NutrEval study ($170) and a Doctor’s Date 24 hour urine mineral
assessment ($60) will help us understand the functional significance of your
Methyl Cycle alleles, and will provide information regarding
oxidative/inflammatory stress, and give us Co-Enzyme Q10 and glutathione
levels. In the future we may wish to remeasure SAMe and SAH. The Health
Diagnostics and Research Institute (www.hdri-usa.com - $350) can give us levels
of SAMe, SAH, and folic acid derivatives (which will help us understand the
affects of your MTHFD1 and DHFR alleles). Alternately, Doctors Data gives us a
less extensive but still useful Methylation Panel for $155. A Sanesco study
($90) will give us salivary cortisol values and urine neurotransmitter
(serotonin, dopamine, etc.) values.
10. After urine sulfate levels fall to 400-800, we may wish to advance
supplementation with methyl-B12 or possibly add in SAMe or BH4 in a step-by-step
fashion.
11. Be self-observant and keep records. Which foods, supplements, or other
maneuvers increase or decrease your sulfate spill? Which make you feel better
or worse? Always keep in mind that detoxification is not a fun experience. You
may need to accept some transient fatigue, malaise, and achiness to allow toxic
molecules to be cleared. Conversely, if detox symptoms are debilitating or
compromise your ability to work or care for your family, then we need to back
off on your treatments. Balance needs to be achieved. Rectifying your genomic
predispositions and detoxifying your system is not a sprint – it is a marathon.
And, as your genes are not going to change, and as the environment is not going
to become less toxic, you will need to be mindful of these principles for the
rest of your (long and healthy) life.
* How tightly should you restrict dietary protein? The degree of protein restriction best suited for you will be in relation to your personal health characteristics and your clinical and biochemical (urine sulfate and ammonia levels) response to treatment. We need to keep in mind that Methyl Cycle Genomics is not the sole determinant of your health. A low protein diet could become a high carbohydrate, weight gain diet in an overweight individual with adult onset diabetes, nor do we wish to create an essential amino acid deficiency. Individuals with chronic, unexplained illness or significant toxicity would do well to follow the “nothing with eyes” diet until urine sulfate and ammonia levels have fallen; later on we will liberalize your diet, while keeping an eye on these biochemical markers. This maneuver isn’t fun and will require personal strength, but it also may turn your health around. Individuals in whom the CBS up regulation is less important (A360A as opposed to C677T, lower urine sulfate and ammonia levels, and better overall health), could simply cut back on animal protein. In addition, the greater representation of ammonia reducing (Yucca, Charcoal, Sparga, Ammonia Support RNA) treatments in your program, the more protein you will be able to take in without compromising your biochemistry. This is all about balancing diet against treatment response. Please do not make radical changes in your diet based solely upon our analysis of your genomic status. Pay attention to and think about these recommendations. The results of the above recommended lab studies will tell us more about the functional expression of your genes and this will guide us with respect to how tightly you should restrict dietary protein and sulfate/sulfite containing meds and supplements.
** The point of Methyl Cycle analysis/treatment is
to help you become a more efficient detoxifier. Toxicity testing (discussed in
more detail in other presentations and on heartfixer.com) thus makes sense.
This could take the form of:
A. The NutrEval provides us some information regarding organic pollutants and
gives us red cell (reflecting what your physiology has been exposed to over the
preceding three months) toxic metals ($170 with commercial insurance; fully
covered under non-HMO Medicare).
B. The US BioTek study gives us information on seven major organic pollutants
($126).
C. A formal provocative challenge gives us our best assessment of tissue metal
burden ($250).
D. The Hunt Digital picture ($350) approach assesses for toxicity (and other
health challenges) by analyzing the frequencies emitted by your body (and tells
us which Digital Homeopathic Patches would be most appropriate). I can’t prove
this approach with an allopathic lab test but it has been quite helpful in
solving complex medical problems in my personal patients. Dr. Hunts CD is
available for your review and you can go to www.auraexplorationpatches.com for
additional information.
E. While on the subject of energy medicine, learn about the grounding/earthing
concept. This approach is low in cost and likely has value for all of us. My
colleague Dr. Sinatra wrote a book on this subject (heartmdinstitute.com). A
negative field only magnetic sleep pad is also a plus. This concept is covered
in our MME DVD and on Dr. Bonlie’s website magneticosleep.com (as you are
working with me your price for a sleep pad would be discounted).
AN IMPORTANT GOAL WILL BE TO REDUCE YOUR SULFATE STORES
AND DECREASE AMMONIA AND GLUTAMATE GENERATION
Gene by Gene Approach – COMT -/- with VDR Taq +/+ and MTRR +/-
This constellation of alleles is discussed on pages 112-115
of Dr. Yasko’s book, Genetic Bypass. Additional information is available on our
heartfixer.com website. VDR Taq influences dopamine production. Being +/+ for
VDR Taq means that dopamine production is compromised. Being COMT -/- means
that you are breaking down dopamine rapidly and in doing so using up available
methyl groups, compromising your ability to deal with toxins and microbes (thus
you are more likely than COMT +/- or COMT +/+ individuals to bear a metal
burden). You need and should tolerate dopamine precursors and methyl donors.
COMT (Catechol-O-Methyl Transferase) inactivates catecholamines (dopamine,
norepinephrine, and epinephrine). Caffeine and stress increase catecholamine
production. Individuals with genomic or acquired COMT dysfunction are thus more
sensitive to their effects. Stated otherwise, high coffee intake increases
cardiovascular risk in COMT +/+ individuals but not in those with normal COMT
status, and caffeine induced insomnia will be more of an issue in those with
COMT +/+ than COMT-/- status. COMT is also involved in estrogen metabolism,
mediating generation of the anti-cancer, anti-vascular disease 2-methoxy
estrogens (see Estrogen Metabolism section of website) and inactivation of the
stronger, potentially genotoxic 4-hydroxy and 16-hydroxy estrogen molecules.
Endogenous and caffeine induced catecholamines, estrogen molecules, and
quercetin “compete” for COMT mediated methylation. This is not an issue in COMT
-/- individuals, as there is plenty of COMT function to go around, but when COMT
function is limited (COMT +/+ individuals have only 25% the O-methylating
capacity of COMT -/- individuals), competition becomes more of an issue. This
explains how stress and caffeine increases risk of cardiovascular disease and
reproductive organ malignancy to different degrees in different people
(genomic-environment interaction). While estrogens, quercetin, and
catecholamines “compete” for the attention of COMT, S-Adenosyl Homocysteine
(SAH) serves as a “non-competitive” COMT inhibitor. S-Adenosyl Methionine
(SAMe) donates the methyl group that COMT uses to O-methylate its substrate,
producing an O-methylated substrate and SAH. SAMe and SAH compete for the SAMe
binding site on the COMT molecule (think of the SAMe binding site as the
“on-off” switch for COMT). A build up of SAH will thus turn down COMT
activity. When Homocysteine builds up, SAH builds up behind it. COMT metabolic
dysfunction, with secondary inability to metabolize catecholamines and estrogen
molecules, is a key mechanism through which elevated homocysteine damages our
health. Unmetabolized catecholamines and estrogen molecules generate oxidative
stress, leading to vascular and neurological disease. Unmetabolized estrogen
molecules damage DNA, increasing risk of breast and prostate malignancy. While
elevated Homocysteine is always deleterious to overall health, high Homocysteine
in the presence of COMT dysfunction is a metabolic disaster.
Your COMT pathway is likely wide open as you are COMT -/- and your
homocysteine level is OK at 9.8 (and we will check your SAMe and SAH levels in
the future).
MTR uses 5-methyl folate and methyl-B12 to convert
homocysteine in to methionine. Being MTRR +/- you are having some trouble
converting B12 into methyl-B12, a problem that is biochemically easy to overcome
with methyl-B12 supplementation.
COMT -/- individuals can utilize methyl groups efficiently, and thus
methyl group supplementation is not likely to lead to irritability (as it might
in COMT +/+ individuals). Dr, Yasko feels that VDR status effects dopamine
generation. As you are COMT -/- and VDR +/+ you should tolerate methyl group
supplementation well. Stated otherwise, as you are
COMT -/- and VDR +/+, you are making less dopamine in response to Vitamin D and you are breaking dopamine down rapidly. Thus you need and should tolerate methyl donors such as Methyl-B12, TMG, melatonin, curcumin, SAMe, or MSM (the only caveat here is that if urine sulfate is high, additional methylated B vitamin, SAMe, and MSM may tip you into a sulfite/sulfate excess situation – thus we do not wish to push here until urine sulfate levels are under control). If dopamine levels are low (we can check urine dopamine with the Sanesco study), you might benefit from quercetin (inhibits COMT) or macuna puriens (raw material for dopamine), or the Sanesco Procite-D preparation.
By stimulating BHMT, we can bypass any block that MTRR places on homocysteine detoxification, and this maneuver will also draw methyl cycle intermediates away from sulfate/sulfite production. Trimethylglycine directly stimulates BHMT, and its use makes sense. BHMT is zinc dependent and we plan on checking your zinc status with a 24 hour urine mineral assessment. PhosChol (already on board) provides phosphatidyl choline which stimulates BHMT. DetoxMax (Lipophos EDTA) provides phosphatidyl choline to stimulate BHMT and EDTA to remove lead (which compromises function of multiple enzymes, whether they are genetically normal or abnormal, including GAD, which converts glutamate in to GABA) and cadmium (which contributes to hypertension and cancer risk).
If you are troubled by agitation or anxiety (perhaps on the basis of excessive glutamate production due to a CBS up regulation), we can address this with GABA or Zen (GABA + Theanine). As you are COMT -/- and VDR Taq +/+, you should tolerate and benefit from the methyl groups provided by theanine. However, if agitation occurs, suggesting methyl group excess, we can utilize GABA, which does not contain methyl groups (both GABA and theanine stimulate the GABA receptor, and thus provide a “Valium” like effect without concern for drowsiness or dependency). Neither GABA or Zen work quickly (we have other supplements for “as needed” use) and are best taken twice a day as a nutritional approach to combat the biochemical consequences of stress (emotional or glutamate-induced stress). Other approaches to dealing with an imbalance between glutamate and GABA include avoiding glutamate rich food products (see appendix III) and supplementation with grape seed extract 100 mg/day and/or (if a CBS up regulation is not present) taurine 500 -1000 mg/day. DetoxMax (Lipophos EDTA) provides phosphatidyl choline to stimulate BHMT and EDTA to remove lead (which compromises function of multiple enzymes, whether they are genetically normal or abnormal, including GAD, which converts glutamate in to GABA). EDTA efficiently removes lead and cadmium, and has activity against aluminum, nickel, and arsenic. EDTA is not an efficient mercury chelator. EDTA is typically well tolerated in individuals with a CBS up regulation.
Plan of action for COMT -/- with VDR Taq +/+, and MTRR +/-
1.
Hydroxy-B12 is already on board to stimulate SUOX. If MMA is high on your
NutrEval we will add in methyl-B12 (to bypass the MTRR +/- block on Methyl-B12
production).
2. Phosphatidylcholine (PhosChol 900 mg/day) to stimulates BHMT and spare SAMe
(much of our SAMe is “spent” generating phosphatidylcholine) is already on
board; as you are +/+ for PEMT please increase to 900 mg twice a day. Later, if
we feel that metal detoxification is appropriate we could switch to low dose
Lipophos EDTA (removes lead, cadmium, and aluminum). Please add TMG 750 mg
twice a day to directly stimulate BHMT.
3. A Sanesco study will give us urine dopamine (and other urine
neurotransmitter) levels and will tell us if dopamine support is needed, and the
NutrEval will give us levels of the dopamine precursors tyrosine and
phenylalanine.
4. If dopamine is low (and I suspect it is, as this a drive towards
mind-altering substance use) we could intervene with:
A. Quercetin Plus, to blunt dopamine degradation by COMT.
B. After one to two weeks of Quercetin Plus we could add Sanesco Procite-D.
C. Depending upon your response, we could later add SAMe 200 mg/day or Sanesco
Methyl Max, and later we could add BH4 2.5 mg/day – a step-by-step approach
makes sense here.
5. We know that your Vitamin D nutriture is
OK
MTR (Methionine Synthase) transfers a methyl group from Methyl-folate to Homocysteine to form Methionine. MTRR (Methionine Synthase Reductase) adds the Methyl group to otherwise inactive B-12. MTRR abnormalities compromise the generation of methyl-12. Without methyl-B12, MTR cannot use methyl-folate to recycle homocysteine into methionine.
VDR Taq status compromise the production of dopamine. COMT -/- (normal function) allows rapid breakdown of the dopamine you can generate. VDR Taq+/+ with COMT -/- individuals will experience low dopamine levels (with consequent increased sensitivity to metal overload) and will benefit from dopamine precursor therapy and from methyl group donors.
Gene by Gene Approach – MTHFR C677T +/-
Here ½ (+/-) of your MTHFR enzymes are having trouble converting 5,10-methylene THF into 5-methyl folate. Without 5-methyl-folate (which we will shorten to methyl-folate) MTR cannot detoxify homocysteine in to methionine. Methyl folate has another role - it can neutralize peroxynitrite. When NOS (nitric oxide synthase) is not functioning normally (i.e. when BH4 is deficient), arginine is converted not in to the vasoprotective molecule nitric oxide, but rather in to the damaging free radicals superoxide and peroxynitrite. Superoxide (neutralized by Vitamin C) can further degrade nitric oxide, while peroxynitrite degrades BH4 (stimulating a vicious cycle). Methyl folate can neutralize peroxynitrite, thus sparing BH4, keeping it available such that NOS can generate nitric oxide, the vasoprotective molecule that we need - thus the need to maintain healthy production/levels of methyl folate. In addition, supplemental methyl-folate can be “back converted” in to folate and then to DHF (dihydrofolate), in this process “recharging” spent BH2 back into useful BH4. Methyl-folate can also “stand in” for BH4 when the later is in short supply. Methyl-folate is thus an extremely important biomolecule. We can easily bypass the MTHFR C677T block with 5-methyl folate supplementation. Sources of 5-methyl folate include Folapro (800 mcg 5-methyl folate), Metanx (5-methyl folate 2.8 mg, P5P 25 mg, and methyl-B12 2 mg), Deplin (7.5 mg 5-methyl folate), and Cerafolin NAC (5-methyl folate 5.6 mg, NAC 500 mg, and methyl-B12 2 mg). Riboflavin deficiency may be a key issue in individuals with C677T alleles, as this SNIP codes for a MTHFR enzyme that does not bind well to its FAD (riboflavin based) co-factor. Individuals +/+ for MTHFR C677T with above average riboflavin nutriture typically have normal homocysteine levels, while individuals low in riboflavin and + for C677T will have the highest homocysteine values. We can assess for riboflavin and folate sufficiency with NutrEval testing. Serum homocysteine gives us information regarding methyl-folate sufficiency (keeping in mind that individuals with CBS up regulations may have low homocysteine levels even in the presence of methyl-folate and/or methyl-B12 insufficiency)
Gene by Gene Approach and Plan of Action – MTHFR A1298C +/+
Dr. Yasko describes MTHFR A1298C as an abnormality in the SAMe binding site of MTHFR that compromises the “backward reaction” that generates BH4, a problem in that BH4 is being used up detoxifying ammonia (which you are making in excess due to your CBS up regulations). This “backward reaction” is not supported by other authors, but a pathway does exist (mediated by DHFR) such that poor methyl-folate status will compromise BH4 recycling. Methyl folate supplementation may stimulate the backward reaction and will help regenerate BH4, and methyl-folate can “stand in” for BH4 when the latter is depleted. After your urine sulfate levels have fallen we may advance methyl-folate or add in BH4 supplementation. If we supplement aggressively in the presence of high urine sulfate, patients may feel great for one day and then experience an incomplete detox reaction. As you are already on methyl-folate I do not think you need to stop it but we will not increase the dose until sulfate levels are under control (< 800). Sauna increases BH4 production and promotes detoxification and could be utilized.
Plan of Action – MTHFR C677T and 3 and MTHFR A1298C all +/-
1. When urine sulfate levels
fall to < 800 please add 400 mcg/day of methyl-folate to your program. Two weeks
later, if urine sulfate stays < 800 and you are feeling well please advance the
dose to 800 mcg/day.
2. Please add riboflavin 100 mg/day to your program, and we will assess your
riboflavin status with NutrEval testing.
3. Another idea – Far Infrared Sauna promotes detoxification and increases BH4
levels.
Gene by Gene Approach – SHMT +/-
SHMT combines the amino acid serine with folic acid to form 5,10-methylene THF, which is used to generate the building blocks for DNA and RNA generation. We can bypass this block with 5-formyl THF, also known as Folinic acid.
Plan of Action – SHMT +/-
As you are +/- and not +/+ for SHMT please add 5-formyl THF, also known as folinic acid, 400 mcg daily (or 800 mcg every other day) to your program. If all goes well please increase to 800 mcg/day in two weeks.
Gene by Gene Approach and Plan of Action – SLC19A1 +/+
SLC19A1 is
involved in transport of folates in to our cells, a problem that we can address
with methyl-folate and folinic acid supplementation.
Gene by Gene Approach and Plan of Action – MTHFD1 +/-
The trifuncitonal enzyme, 5,10-methylenetetrahydrofolate dehydrogenase/ 5,10-methylenyltetrahydrofolate cyclohydrolase/ 10-formyltetrahydrofolate synthetase (MTHFD1) is responsible for the conversion of 5,10-methylene THF (generated from THF by SHMT) to the corresponding 10-formyl, 5,10-methenyl and 5,10-methylene derivatives (and you are low here). A common mutation at position 1958 within the MTHFD1 gene results in a transition of guanine to adenine (G>A) that may result in a reduction in folate metabolism. Our approach here involves general support of the Methyl Cycle and the inclusion of methyl-folate and folinic acid in to your program.
Gene by Gene Approach and Plan of Action – DHFR +/-
Here you are having some trouble reducing oxidized dietary folates into useful Tetrahydrofolate, and in recycling “spent” BH2 back in to useful BH4. Our approach here involves methyl-folate and folinic acid supplementation (as per the MTHFR recommendations).
Gene by Gene Approach – MAO A +/-
MAO breaks
down serotonin and to a lesser extent dopamine and norepinephrine. This
disorder is associated with an increased tendency to mood swings and panic
disorders, related to fluctuations in serotonin levels. Serotonin formation may
pick up as BH4 levels are restored with other maneuvers to address methyl cycle
abnormalities. Tryptophan in food is converted into serotonin and tyrosine in
food in to dopamine. If one is abnormal for MAO and normal for COMT, then
emphasizing foods higher in tyrosine than in tryptophan makes sense (however,
our initial goal is to lower sulfate, so the recommendation to avoid animal
protein overrides the recommendation to take in foods high in tyrosine).
Gene by Gene Approach – Methyl Thieves and SAMe Stealers
A key goal of Methyl Cycle physiology (and a focus in our work with you) is to
ensure sufficient, replenishable, and physiologic (not excessive) supplies of:
A. SAMe, along with and an appropriate SAMe to SAH ratio (it is the ratio, not
just the SAMe level, that drives forward useful methylation reactions).
B. BH4 (needed to generate neurotransmitters and nitric oxide).
C. Key antioxidant and detoxification molecules (glutathione, taurine, sulfate,
and cysteine).
D. Purine and Pyrimidine bases for DNA and RNA generation.
You are generating (or taking) methyl folate and methyl B12, not for the sake of generating high levels of these Methyl Cycle intermediates (yes, intermediates, not finished products), but rather to help ensure that the Methyl Cycle work products (SAMe, BH4, glutathione, cysteine, and taurine) are in adequate supply.
While our focus has been on improving SAMe supply, we should also consider means to reduce SAMe expenditure (Mother Nature balances supply and demand – the government should pay heed)! Stated otherwise, if nutritional supplementation decreases demand for SAMe, more will be available to meet critical demands (e.g. DNA methylation to silence inflammatory and proto-oncogenes).
So how are we “spending” SAMe? What phenomena lead to SAMe wasting or diversion? How do we ameliorate these pathophysiologies to restore SAMe and appropriate SAMe:SAH balance?
In considering SAMe expenditure, remember that each time we “spend” a SAMe (S-Adenosylmethionine) to carry out a specific methylation reaction, we create a SAH (S-Adenosylhomocysteine), which in turn inhibits methylation. A declining SAMe:SAH inhibits methylation reactions; it does us no good to increase SAMe if at the same time we buildup SAH.
Fortunately, SAH is rapidly converted to Homocysteine and Adenosine. Adenosine is efficiently removed, but if the Methyl Cycle is sluggish, due either to SNIPS, toxins, or nutritional deficiency, Homocysteine will build up. Homocysteine will then be back converted to SAH, the SAMe:SAH ratio falls, and useful methylation grinds to a halt. Homocysteine itself is not the problem; it is the buildup of SAH, compromising methylation potential, which leads to disease states such as atherosclerosis, cancer, and mood disorders.
So what processes “steal” SAMe? In considering this issue,
we need to be aware that CBS (which irreversible drains Homocysteine down the
trans-sulfuration pathway and away from SAMe reformation) is up regulated
(enzymatic activity increases) by oxidative stress and inflammation.
A. Oxidative stress:
When the generation of free radicals (superoxide, hydroxyl, and hydrogen
peroxide) outpaces our ability to neutralize them with endogenous (e.g.
superoxide dismutase) or exogenous (supplemental antioxidants), we suffers from
a buildup of free radicals. To address this immediate threat to health,
Homocysteine metabolism down the CBS pathway (irrespective of SNIP status) will
increase. Homocysteine (and with it the potential to create new SAMe) will be
irreversibly diverted away from remethylation (via MTR and BHMT back into
methionine for conversion to SAMe) and towards the production of glutathione,
taurine, and cysteine.
This all makes sense. Oxidative stress damages our physiology and kills cells. When faced with oxidative death, it makes sense to divert Methyl Cycle resources towards antioxidant generation. After oxidative stress has been neutralized, CBS flow will decrease, Homocysteine will start flowing back towards SAMe, and useful methylation reactions will resume. Our problem is that most ill Americans suffer from unremitting oxidative stress (we can measure your individual level of oxidative stress with the NutrEval study). Homocysteine will thus be shunted down the CBS pathway, such that useful methylation of DNA, estrogen molecules, and catecholamines will be compromised. If you cannot methylate catecholamines, then oxidative stress will develop within your blood vessels. If you cannot methylate your DNA, than you cannot silence inflammatory genes. You thus make more inflammatory molecules, more free radicals build up, more Homocysteine is diverted away from SAMe regeneration, and you are now chronically ill.
The solution is to undergo an assessment of oxidative stress, and then takes steps to resolve any challenges present. This will involve removing from your body phenomena that generate free radicals (e.g. smoking, toxic metals, organic pollutants) while concomitantly shoring up your antioxidant defenses with nutrients that we find to be in short supply (selenium, Vitamin E, Vitamin C, etc.). We can thus use nutritional medicine to help you generate SAME and to prevent oxidative stress from “stealing” Homocysteine away from SAMe regeneration. As a side note, toxic metals not only “steal” SAMe, they also compromise its formation (e.g. Mercury compromises MTR, in this fashion blocking useful remethylation of Homocysteine back into methionine for conversion into SAMe).
B. Inflammation: Inflammatory TH1/TH17 cytokines, such as TNF-alpha, Il-6, and Il-1b also increase flow down the CBS pathway, draining Homocysteine away from useful remethylation back in to SAMe. Inflammation leads to oxidative stress and oxidative stress leads to inflammation. Both are useful in fighting infection, but both processes are persistently elevated as our immune system misinterprets as infection the chronic “pseudoinfections” of visceral obesity, leaky gut, and environmental toxicity. Thus by resolving inflammation (either with anti-inflammatory nutrition interventions such as turmeric or berberine) or by removing the cause of chronic inflammation (weight loss or resolving leaky gut) we can resolve the “inflammatory drain” on SAMe supply and demand. Your inflammatory cytokines were not elevated in 2014.
What processes deplete our SAMe stores? Are some less critical than others? Can we decrease SAMe demand with nutritional supplementation?
A. DNA methylation: This is sacrosanct. Only SAMe can methylate DNA. Only SAMe can shut down the transcription (reading into protein formation) of viral, inflammatory, and proto-oncogenes (promote cancerous transformation) while maintaining the transcription of tumor suppressing and anti-inflammatory genes. We can’t scrimp on DNA methylation, but by resolving oxidative/inflammatory stress, and supplementing with SAMe “sparers” as described below, we can maintain adequate SAMe (with a high SAMe:SAH ratio) to ensure optimal DNA methylation.
B. Creatine formation: Around 50% of our SAMe is “spent” in the generation of creatine, a molecule critical to energy maintenance. We do work by splitting a high energy bond within ATP (Adenosine Triphosphate) to produce ADP and phosphate. We burn carbon and use this energy to rephosphorylate ATP. When energy is plentiful, ATP will transfer a phosphorus group to creatine, forming Phosphocreatine. Should we suddenly run out of ATP energy (sprinting, weight lifting, or if oxygen supply:demand is compromised by a blocked artery or failing heart), Phosphocreatine can download a high energy phosphate bond back to ADP, regenerating ATP such that cellular work can continue. We actually store 10 heart beats of energy as Phosphocreatine. As you would expect, creatine supplementation has been shown to be helpful in anaerobic athletic performance as well as in heart failure. Of interest, creatine has been shown to lower cholesterol, and while the literature is not 100% consistent, creatine supplementation will decrease expenditure of SAMe and increase the SAMe:SAH ratio. Athletes take 5 grams of creatine, four times a day (saturation dose) for one week, followed by 5 grams/day (maintenance dose). However, unless you have an athletic competition coming up, you can simply add 5 grams of creatine/day to your program. Creatine is not unsafe, but there have been instances where competitive body builders dosed up on creatine while decreasing fluid intake (so their muscles will bulge out more) leading to dehydration and kidney compromise. Creatine is converted in to Creatinine, which is filtered out by the kidneys. We use serum creatinine to gauge kidney function. A trivial rise in serum creatine may occur when you supplement with creatine. This does not mean that kidney function is decreasing; rather this is an artifact due to creatine supplementation. Creatine supplementation at 5 grams/day makes sense for individuals with Methyl Cycle SNIPS that might compromise SAMe generation or maintenance (MTHFR, MTR, and BHMT), or when we feel that chronic oxidative/inflammatory stress is depleting SAMe regeneration.
C. Phosphatidylcholine: Three SAMe molecules, around 30%
of our total supply, are used to methylate phosphoethanolamine into
phosphatidylcholine. Phosphatidylcholine (PC) is involved in lipoprotein
formation and reverse cholesterol transport; PC is also a critical component of
the cell membrane. The common name for PC is lecithin. PC/lecithin is
essentially a triglyceride like molecule with two fatty acids and one
phosphocholine group attached to a three carbon glycerol backbone. The
biochemical utility of PC relates to the composition of its two fatty acids. PC
containing two unsaturated linoleic acid molecules (polyenylphosphatidylcholine)
is used IV and orally to treat cardiovascular, liver, and neurological disease
(see our DVD presentation). If we supplement you with PC, less SAMe will be
spent generating PC, and more will be available for useful methylation
reactions. In addition, the less SAMe spent, the less SAH and Homocysteine will
be formed. Furthermore, PC can be converted into choline, which can be
converted into Betaine (TMG or trimethylglycine) which is used by BHMT to
directly remethylated homocysteine back in to methionine (which is then
converted in to SAMe). Thus PC supplementation will lower an elevated
Homocysteine and increase SAMe supply along with the SAMe:SAH ratio. We use
PhosChol (unsaturated phosphatidylcholine rich in linoleic acid) 900 to 2700
mg/day in the treatment of cardiovascular and liver disease. Our dose in Methyl
Cycle patients will relate to your SNIP status and baseline Homocysteine level.
Being +/+ for PEMT, you are having trouble generating phosphatidylcholine,
which we will address with phosphatidylcholine supplementation.
D. COMT utilization. COMT (Catechol-O-Methyl transferase) metabolizes estrogen molecules, catecholamines (dopamine and norepinephrine), drugs (e.g. L-Dopa used in the treatment of Parkinson’s disease) and bioflavonoids (particularly Quercetin) by transferring a methyl group from SAMe to an oxygen molecule on the compound being methylated. Each time this occurs, SAH is generated, the SAMe:SAH ratio falls, and COMT and all other methyl-transferase enzymes are inhibited. If we are interested in sparing SAMe and maintaining a high SAMe;SAH ratio, it would be prudent to reduce the need for COMT-driven methylation. Lowering stress will lower norepinephrine, and thus decrease SAMe utilization by COMT. While bioflavonoids such as Quercetin have many beneficial properties, if SAMe preservation is critical (high Homocysteine in the presence of MTHFR, MTR, MTRR, and BHMT SNIPs or if our ability to methylate estrogen molecules is impaired) then decreasing intake of Quercetin and related bioflavonoids would be prudent. Conversely, when insufficient dopamine is the problem, we might use Quercetin to blunt dopamine degradation by “clogging up” COMT. Caffeine increases catecholamine production. Caffeine intolerant individuals are typically COMT +. When caffeine intolerance develops anew, we look for new problems that might be compromising SAMe supply or COMT functionality.
Plan of action
for Methyl Thieves and SAMe Stealers )
1. Evaluate
for the presence of oxidative and/or inflammatory stress and take corrective
action. A Genova Labs NutrEval study will be quite helpful in this regard.
2. Creatine 5 grams/day (mixed in a liquid) to spare SAMe.
3. PhosChol, 900 mg, twice a day, to spare SAMe and promote homocysteine
methylation.
Gene by Gene Approach – SOD3 +/+ and SOD2 +/+
SOD3 refers to extracellular superoxide dismutase, which protects the vascular endothelial lining and nitric oxide synthase from oxidative stress. SOD2 protects the mitochondria from oxidative stress and is dependent upon adequate manganese nutriture. Your NutrEval study will tell us whether you are or are not experiencing oxidative stress. To my understanding, Co-Enzyme Q10 and Vitamin C (and presumably any maneuver that decreases oxidative stress will increase SOD3 activity. GliSODin (available in Life Extension Endothelial Defense) will do the same and has been shown to have a favorable affect on atherosclerosis (favorable affect on carotid IMT). Pharmaceutically, ACE inhibitors and ARB (angiotensin receptor blockers) will increase SOD3 activity.
Plan of Action – SOD3 +/+ and SOD2 +/+
1. If we
identify oxidative stress on your NutrEval than Life Extension Endothelial
Defense 1-2 daily would make sense.
2. We will make sure that manganese, zinc, and copper nutriture is adequate (24
hour urine mineral assessment).
Gene by Gene Approach and Plan of Action – NAT2 +/+
N Acetyl Transferase is involved in the activation and deactivation of arylamine and hydrazine drugs and carcinogens. You are +/+ for a down regulation and +/+ for an up regulation. NAT can be supported with N-Acetyl Cysteine, B vitamins B2, B3, B5, and Mb. Nutritional testing will tell us whether these co-factors are in sub-optimal supply.
Gene by Gene Approach – NOS3 +/+
NOS (Nitric Oxide Synthase) in a BH4 dependent reaction, converts Arginine in to Nitric Oxide, our most important vasoprotective molecule. NOS is also involved in ammonia detoxification. Our treatment here includes previously described efforts to lower your ammonia burden, our general cardiovascular treatments designed to improved endothelial function (which is dependent on nitric oxide) and the addition of BH4 to your program after urine sulfate levels have fallen. We can measure endothelial function in the office with EndoPAT testing.
Gene by Gene Approach and Plan of Action – CPOX4 +/-
This SNIP renders you more sensitive to metabolic impairment on the basis of mercury exposure. Do you bear mercury amalgam fillings? Did your mother? We will assess your tissue metal burden and in the future begin a detox program, likely not involving sulfhydryl group bearing chelators such as DMPS and DMSA. QuickSilver, the Battle Plan, and DetoxMax would likely be better tolerated.
Gene by Gene Approach and Plan of Action – BDNP +/- and NTRKS +/+
These SNIPs are likely associated with reduced BDNP (Brain Derived Neurotrophic Factor). BDNP is neuroprotective and lower levels/reduced function is associated with reduced mood and increased susceptibility to mercury. I need to do more reading on this gene tandem. Overall, from a genomic basis you appear to be sensitive to mercury.
Gene by Gene Approach – ACE +/-
Angiotensin II activity is up regulated, predisposing you to hypertension and increasing your risk for atherosclerotic vascular disease. If drug therapy is needed for hypertension, the best agents will be tissue specific ACE inhibitors (Quinapril, Ramipril) and/or Spironolactone, a relatively weak diuretic that blocks the action of Aldosterone, which when up regulated plays a role in the development and progression of heart disease and heart failure. An angiotensin receptor blocker (ARB) serves as an alternative approach. Of interest, individuals with this genotype respond to statin therapy with greater drops in LDL and more pronounced blunting of plaque progression than do ACE -/- individuals. ACE may cause anxiety, which could be addressed with the Anxiety Support RNA product.
Gene by Gene Approach – ADIPOQ +/-
Adiponectin is a beneficial adipokine (signaling molecule released from fat cells) that promotes insulin sensitivity and protection against vascular disease. Genomic down regulations in Adiponectin do not have a major effect on Adiponectin expression, while life style and environmental factors do. Adiponectin expression is increased with exercise, reduction in visceral adiposity, magnesium, EPA (more than with fish oil), moderate alcohol intake. Pharmaceutical agents that increase adiponectin expression include ACE inhibitors, ARBs, thiazolodinedione insulin sensitizers, and fibrate lipid lowering agents. Oxidative and inflammatory stress, visceral adiposity, smoking, high catecholamine levels, and high cortisol all decrease adiponectin expression. We can measure adiponectin within the Boston Heart profile.
Gene by Gene Approach – NR3C1 +/-
This SNIP renders you more sensitive to the effects of glucocorticoids, such as cortisol and prednisone, predisposing to HPA axis (“adrenal fatigue”) dysfunction. Do you and Dr. Smith feel you are getting enough cortisol support? You probably are. If not we could check salivary cortisol values (within the Sanesco study).
Gene by Gene Approach and Plan of Action – CYP1A1 and 1A2 +/+
CYP1A1 and 1A2 +/+ (down regulation) status means that your ability to 2-hydroxylate estrogen molecules will be compromised. On a positive note, you do not bear a CYP1B1 up regulation that would promote conversion of estrogens down the 4-hydroxylation pathway. As you are COMT -/-, you should be able to methylate estrogen molecules properly. At some point a 24 hour urine for estrogen hydroxylation and methylation status could be carried out.
Phase I detoxification of hydrocarbon pollutants (air pollutants, smoking, charred meats) will also be compromised. We can stimulate 1A1 and 1A2 activity with DIM, I-3-C, and Sulforaphane (keeping in mind their sulfate/sulfite content).
CYP1A2 +/+ (down regulation) status also compromises your ability to degrade caffeine, which itself stimulates the adrenal gland to release catecholamines, which in turn must be broken down by COMT, the function of which in you is unimpaired.
Gene by Gene Approach and Plan of Action – CYP2D6 C2850C +/+
This SNIP codes for increased activity of this enzyme. You may require higher doses of agents that are metabolized by CYP2D6 to obtain the desired pharmaceutical effect.
Additional Thoughts
1. The above are general recommendations, based upon my review of your Methyl
Cycle Genomic status and the history provided. Lab testing will tell us how
these genomic predispositions (genotype) are expressing themselves within your
physiology (your phenotype), and I will have much more to say based upon your
laboratory assessment. The 24 hour urine mineral and Genova NutrEval studies
make sense, along with a serum iodine level. The Sanesco study will be helpful
but is not critical. We should delay the Drs. Data Methylation Panel until your
program has been in place for several months.
2. Please make sure that my recommendations do not run counter to the plans of
your other physicians (not likely but we certainly do not want to create a
treatment conflict).
3. We can discuss all of this after your have had a chance to read
through my write-up (we could set up a brief or full phone consultation or an
office visit – perhaps a brief discussion to go over the original plan and a
more in depth conversation after lab studies have returned).
4. Your analysis contains more information than do my usual reports (I
researched some of the SNIPs, thus the delay in getting back to you). As such,
would it be OK with you if I posted your report (anonymously) on the
heartfixer.com website?
James C. Roberts MD FACC FAARFM
4/28/15
Sample Report - Adult with Fatigue and Chemical Sensitivity
|
Nutrigenomic Report - 46 y/o Female |
||
|
Methylation Panel Abnormalities for Genes with Characterized SNIPs |
||
|
Gene Name |
Variation |
Finding |
|
COMT |
V158M |
Homozygous (+/+) |
|
COMT |
H62H |
Homozygous (+/+) |
|
COMT |
P199P |
OK |
|
VDR |
Bsm |
Heterozygous (+/-) |
|
VDR |
Taq |
Heterozygous (+/-) |
|
MAO A |
R297R |
Homozygous (+/+) |
|
ACAT |
1-02 |
OK |
|
MTHFR |
C677T |
OK |
|
MTHFR |
3 |
OK |
|
MTHFR |
A1298C |
Homozygous (+/+) |
|
MTR |
A2756G |
OK |
|
MTRR |
A66G |
Heterozygous (+/-) |
|
MTRR |
H595Y |
nc |
|
MTRR |
K350A |
OK |
|
MTRR |
R415T |
nc |
|
MTRR |
A664A |
Heterozygous (+/-) |
|
BHMT |
2 |
OK |
|
BHMT |
4 |
nc |
|
BHMT |
8 |
Heterozygous (+/-) |
|
AHCY |
1 |
Heterozygous (+/-) |
|
AHCY |
2 |
nc |
|
AHCY |
19 |
Heterozygous (+/-) |
|
CBS |
C699T |
Heterozygous (+/-) |
|
CBS |
A360A |
Heterozygous (+/-) |
|
CBS |
N212N |
nc |
|
SHMT |
C1420T |
nc |
Overview
The function
of the Methyl Cycle is to maintain (current health status) appropriate levels
of:
A. SAMe, along with a high SAMe:SAH ratio, necessary for biological methylation.
B. BH4, need to generate neurotransmitters and nitric oxide.
C. The antioxidant/detoxification molecules cysteine, taurine, sulfate, and
glutathione.
Your Methyl Cycle and Detox Genomic findings are significant. My hypothesis is that these genomic predispositions have set you up for organic pollutant and metal toxicity and stressed your nutritional status. Overall my thought would be to address your genomic predispositions, optimize your nutritional status, hopefully improve your energy level and sense of well being, and then to initiate a slow but steady detox program that you can tolerate.
You are +/- for both of the CBS up regulations and +/- for at least one of the three BHMT alleles (which act like CBS up regulations - no call means that for technical reasons 23and me could not determine the status of a particular allele). Homocysteine (and its Methyl Cycle precursors) is thus being drawn down the trans-sulfuration pathway, in this process generating excessive sulfur break down products (sulfite and sulfate, which stimulate the stress/cortisol “fight or flight” response; your sulfate levels are 800-1200), too much excitotoxic glutamate (which you may have trouble converting in to GABA due to your GAD1 +/+ status; however your glutamate level was not elevated on your 9/12 NutrEval), and too much ammonia (which depletes BH4, leading to insufficient dopamine and serotonin production). This deficiency in BH4 allows NOS (nitric oxide synthase) to convert Arginine in to free radicals as opposed to nitric oxide, predisposing you to hypertension and cardiovascular disease.
Dr. Yasko feels that MTHFR A1298C (+/+) status compromises recycling of BH4 from “spent” BH2. Your DHFR (+/-) status may also compromise BH4 recycling, so with respect to the precious molecule BH4, you are getting hit at both ends – reduced production and increased utilization. After the problems in the trans-sulfuration pathway (CBS and BHMT) have come under control, BH4 or additional methyl-folate as a BH4 precursor/mimic can be added to your program.
Folate molecules serve to transfer methyl groups within our physiology (think of folates as “methyl group taxis”). To become useful, the oxidized dietary folate molecules that we take in must first be reduced to Tetrahydrofolate (THF) by dihydrofolate reductase (DHFR). You are (+/-) for a DHFR reduced function allele, such that conversion of dietary folates in to useful THF may be compromised.
SHMT (serine hydroxyl methyl transferase – you are +/- here), a pyridoxal-5-phosphate (active form of B6) dependent enzyme, tacks on a methyl group derived from the amino acid serine to generate 5,10-MethyleneTHF, which is then converted to 5-methyl folate by MTHFR. 5,10-MethyleneTHF can also be acted upon by MTHFD1,to generate the building blocks for DNA and RNA generation. Being +/+ for MTHFD1, you are having trouble with these steps and in recycling folate derivatives back in to THF. Being +/- for MTHFS, you are having some trouble breaking down folinic acid. We can measure folate metabolites, and supplement you based upon the results, or we could use a combination of low dose folinic acid and methyl-folate.
Being +/+ for FOLR2 (folate receptor) your cells may have trouble taking up folic acid (more so then with methyl-folate), and thus you may benefit from greater than usual levels of methyl-folate. PEMT (which is stimulated by estradiol) uses three SAMe molecules to generate phosphatidylcholine. You are ++ for a loss of function PEMT allele, and thus you are having trouble generating phosphatidylcholine. We use phosphatidylcholine in the remethylation of homocysteine into methionine by BHMT (also pulling homocysteine away from the “CBS drain”), in lipid metabolism, and in the generation of the neurotransmitter acetylcholine. Phosphatidylcholine supplementation makes sense here.
MTR uses 5-methyl folate and methyl-B12 to convert homocysteine in to
methionine, which in turn is converted in to S-Adenosyl-Methionine (SAMe), the
universal methyl donor. You are +/- for one of the MTRR alleles, meaning that
you are having some trouble converting B12 in to methyl-B12, which will be a
little difficult to address with supplementation, as you are +/+ for COMT. COMT
breaks down dopamine, using up methyl groups in the process. As you are COMT
+/+, you will break down dopamine only slowly, a point in your favor as dopamine
helps defend against toxic metals. However, being COMT +/+ renders you
sensitive to methyl groups. Aggressive methyl group supplementation can lead to
fluctuations in dopamine, producing mood swings. Thus we will be ginger with
respect to methyl-B12 supplementation (also, methylmalonic acid, an index of B12
need, was normal on your NutrEval study, as was methionine, which is generated
from homocysteine in a B12 dependent fashion, and thus methylation of B12 is
likely not seriously compromised).
You are +/- for VDR Taq (and VDR Bsm, which acts like VDR Taq), meaning that you are not making enough dopamine in response to Vitamin D (somewhat mitigating your methyl group sensitivity), but +/+ COMT, meaning that you are breaking down dopamine, and using up methyl groups in this process, quite slowly; thus you will not need nor will you likely tolerate dopamine precursor therapy or high dose methyl group supplementation.
MAO A breaks down serotonin. You are +/+ for MAO A, and +/- for MAO B, so you will break down serotonin relatively slowly, and thus you probably do not have a great need for serotonin precursor therapy.
AHCY converts S-Adenosyl Homocysteine (SAH), generated whenever a SAMe is “spent” in to homocysteine. Being +/- for AHCY this reaction may be sluggish, such that SAH levels may build up, and the ratio of SAMe to SAH could fall, compromising your ability to utilize SAMe as a methyl-donor. Our approach here will be to make sure downstream homocysteine is cleared efficiently and to decrease the generation of SAH (likely with creatine and phosphatidylcholine supplementation).
PON1 +/- compromises the antioxidant function of HDL (and our ability to detoxify homocysteine thiolactone, a toxic derivative of homocysteine), and can be addressed with pomegranate intake. CYP1A2 compromises your ability to 2-hydroxylate estrogen molecules, while being +/+ for CYP1B1 you are predisposed towards 4-hydroxylation. However, your 2/16 ratio is OK at 2.8, and Dr. May has you on I-3-C, which stimulates 2-hydroxylation. Dr. May placed you on iodine to promote metabolism of 16-hydroxy estradiol to estriol, and improving your overall antioxidant status should help here as well (we use antioxidants to reduce 16-OH estradiol to estriol). Your COMT +/+ status is limiting conversion of 2-OH estrogen molecules in to the protective 2-methyoxyestrogens. Being +/+ for CYP1A2 you are having trouble breaking down caffeine, and being +/+ for COMT you are having trouble breaking down catecholamine molecules (dopamine and norepinephrine – “adrenalins”), so it is best that you minimize caffeine (especially coffee) intake.
The Gene by Gene sections provide generic information while specific recommendations for you are described in the Plan of Action sections. Approaches that make the most sense to me receive a (Ö). Those that are less critical (or more costly) are designated (+/-). Your Methyl Cycle abnormalities likely predispose you to impaired detoxification, and your evaluation has demonstrated problems with mercury and tin (the primary source of both is likely your prior mercury fillings).
In thinking about your Methyl Cycle status, we need to keep in mind that recommendations based upon Dr. Yasko’s work with autistic kids may be problematic in adults with other genomic or acquired health challenges. Thus we need to keep everything in proper perspective, particularly with respect to diet. I can see how the CBS “nothing with eyes” diet would be problematic for you, given your well characterized food sensitivities. Your work up to date has been incredibly comprehensive. Dr. Smith knows a lot of things that I don’t ands he has a great understanding of your health status. I will be doing a little bit of brainstorming as we discuss your Methyl Cycle status, and have some ideas for you and Dr. Smith to consider.
Gene by Gene Approach – CBS +/- and BHMT +/-
CBS (Cystathionine Beta-Synthase) is discussed on pages 48-53 of Dr. Yasko’s
book, Genetic Bypass. You are +/- (half of your CBS enzymes are abnormal) for
one of the CBS up regulations and +/- for at least one of the BHMT down
regulations (which act like CBS up regulations). Homocysteine (and its Methyl
Cycle precursors) is being drawn down the trans-sulfuration pathway, in this
process generating excessive sulfur break down products (sulfite and sulfate,
which stimulate the stress/cortisol “fight or flight” response), too much
glutamate (which leads to glutaminergic excitotoxicity – a double problem for
you as your GAD +/- status compromises interconversion of glutamate and GABA,
noting however that your glutamate level was not elevated in 9/14), hydrogen
sulfide (to produce brain fog), and too much ammonia (which depletes BH4,
leading to insufficient serotonin and dopamine production. Your ammonia level
was not elevated in 9/14, likely as you are not taking in excessive animal
protein. A deficiency in BH4 allows NOS (nitric oxide synthase) to convert
arginine in to free radicals as opposed to nitric oxide, predisposing you to
hypertension and cardiovascular disease. Being +/+ for MTHFR A1298C and +/- for
DHFR, you are having trouble regenerating BH4, so with respect to the precious
molecule BH4, you are getting hit at both ends – reduced production and
increased utilization. Thus your ability to generate neurotransmitters and
nitric oxide will be compromised. Instead your genomic status predisposes
nitric oxide synthase to generate the free radicals superoxide and
peroxynitrite, which lead to oxidative stress and inflammation. Compounding
this predisposition towards increased production of superoxide, your +/+ status
for SOD compromises your ability to neutralize superoxide, and your +/- status
for GPX and GSTP compromise your ability to neutralize hydrogen peroxide with
glutathione.
I realize that this sounds awful but these are all issues that we can deal with, now that we understand their origin and biological significance.
During normal physiology, metabolic flow down the CBS pathway is designed to generate the important anti-oxidant and detoxifying molecules glutathione (your level is not high, likely as your glutathione reserves are being used up dealing with mercury), taurine (why your taurine level is elevated) cysteine (elevated), and alpha-ketobutyrate (which Dr. Yasko feels can be converted into GABA, a calming neurotransmitter, or glutamate, an excitotoxin; others dispute this position but we typically see elevated glutamate in individuals with CBS/BHMT + alleles). The CBS C677T and A360A genes code for enzyme function that is pathologically up regulated (your ancestors needed antioxidant support more than they needed methylation support; thus these SNIPs which direct homocysteine towards glutathione and away from SAMe regeneration). You thus suffer from “too much of a good thing and way too much of several bad things”.
Oxidative stress (the accumulation of free radicals) increases flow down the CBS pathway, to generate the above listed antioxidants needed to allow the body to respond to an oxidative challenge – a good thing. However, when homocysteine is drawn down the CBS pathway, it is “lost forever” such that it cannot be remethylated and used to regenerate SAMe. In this fashion oxidative stress (something we wish to avoid) leads to reduced SAMe. SAMe itself stimulates flow down the CBS pathway (if you have plenty of SAMe you do not need to worry about recycling it); this is why we advise you not to begin SAMe (or push with measures designed to up regulate SAMe production) until your CBS/BHMT alleles have come under metabolic control.
SAMe has been used to treat lead overload (and presumably will work against mercury), as SAMe stimulates CBS, which inevitably converts homocysteine into glutathione. Could your poor response to SAMe have been a detox reaction + a response to a CBS induction induced sulfite/sulfate burden (as along with glutathione, CBS generates sulfite and sulfate)?
While sulfate and sulfhydryl (-SH) bearing molecules are important in detoxification, sulfate/sulfite/-SH excess seems to block cellular up take of the key detoxifiers glutathione and cysteine (this is Dr. Yasko’s position; I can’t back this up from my review of the scientific literature but her position seems to work in practice). Endogenous detoxification is thus blunted (nearly all kids with Autism Spectrum Disorders bear CBS up regulations – why they are compromised by environmental toxins and the kid next door is just fine – could this be playing a role in your otherwise difficult to explain health conditions)? Conversely, after we decrease your sulfate/sulfite pool, your detox pathways will open up (and why, if we move too fast, you will experience detox phenomena).
The excess ammonia generated must be detoxified, and to do so BH4 (tetrahydrobiopterin) must be “spent”. This is a problem in that we need BH4 to generate neurotransmitters (serotonin to maintain calm/prevent depression and dopamine to maintain motivation and drive). Without BH4, we cannot convert arginine in to nitric oxide; instead vascular wall toxic free radicals such as superoxide and peroxynitrite are created, leading to hypertension and cardiovascular disease.
Ammonia is metabolized within the urea cycle, an enzyme pathway that utilizes several amino acids (ornithine, aspartate, arginine, and indirectly alpha-ketoglutarate) to break down ammonia. Systemic ammonia detoxification takes place in the liver, and thus individuals with advanced liver disease experience hyperammoniaemia, with attendant neurological dysfunction (tremor, confusion, impaired coordination). We can thus borrow from the gastroenterology community in our approach to the hyperammoniaemia present in our patients with CBS/BHMT/MTHFR alleles (also giving me a chance to consult with our daughter, who is a gastroenterology fellow).
Intestinal microbes generate ammonia. Gastroenterologists use antibiotic therapy (Rifaxamin, a poorly absorbed antibiotic that does not enter the circulation) to sterilize the gut, thus blunting ammonia production. While we may recommend antimicrobial therapy to address bacterial overgrowth demonstrated on a CDSA (Comprehensive Digestive Stool Analysis), our approach will be to take a probiotic 2-3 times a day to promote a balanced intestinal flora (not a bad idea for all of us to deal with the effects of antibiotics found in grocery store meats).
Charcoal seems to absorb ammonia generated within the GI tract, and thus taking charcoal at bedtime seems to lower one’s ammonia burden. Charcoal can also cause constipation, a huge negative here, as moving your bowels 2-3 times a day is important in detoxification and ammonia neutralization. Thus we recommend charcoal three nights a week with magnesium citrate and/or Vitamin C as needed to promote normal GI tract motility (adjust doses to obtain a balance between ammonia neutralization and proper GI tract function – too much magnesium or vitamin C pulls water into the intestines, leading to loose stools and diarrhea). Gastroenterologists utilize the cathartic lactulose to accelerate GI tract motility, blocking ammonia absorption; we can achieve the same end nutritionally with vitamin C and magnesium.
Ornithine/Aspartate supplementation (LoLa), administered IV or orally, has been shown to be a safe and effective approach to ammonia reduction in liver failure, and we can utilize this low cost approach to deal with ammonia excess in Methyl Cycle patients, starting with 1000 mg (1/3rd teaspoon) three times a day, increasing to one teaspoon as needed. Aspartic acid has a glutamate-like stimulating effect, and if one experiences agitation/anxiety than aspartate can be dropped in favor of more ornithine. Ornithine monotherapy has been used to increase exercise capacity in healthy people, as ammonia production is a metabolic consequence of energy utilization. These and other amino acids are best absorbed on an empty stomach or with a carbohydrate; concomitant protein intake will blunt their absorption.
Dr.
Yasko’s diagrams indicate that CBS generates alpha-ketoglutarate, which can be
converted into glutamate. Actually, CBS generates alpha-ketobutyrate.
Nonetheless, individuals with CBS + alleles nearly always display elevated
glutamate, and thus the same physiology holds. We should be able to
interconvert alpha-ketoglutarate into glutamate, glutamine, and GABA. However,
if glutamate is in excess, or if toxic metals compromise the interconversion
enzymes, then we suffer a buildup of the excitatory neurotransmitter glutamate.
Glutamate is involved in alertness and learning, but excess glutamate leads to
irritability and over-excitement; toxic levels may play a role in seizure
activity and cardiac arrhythmia (could this be why we are seeing so much more
atrial fibrillation now then we were ten years ago; MSG, a dietary source of
glutamate, can precipitate atrial fib)? We address high
glutamate/excitotoxicity by avoiding high glutamate/MSG in foods (please see
appendix) and by taking GABA to neutralize the excitatory affects of high
glutamate.
CBS up regulations lead to an initial buildup of potentially neurotoxic sulfite,
which is then metabolized by SUOX (Sulfite Oxidase) to the less neurotoxic (but
still problematic at high levels) sulfate. SUOX activity requires molybdenum,
which is thus depleted in CBS + individuals. Homogenized dairy products contain
xanthine oxidase, which uses up molybdenum, and are best avoided or minimized.
Vitamin E succinate, boron, and B12 are felt to stimulate SUOX activity.
As Methyl Cycle function is needed in the biosynthesis of Co-Enzyme Q10 and
Carnitine, individuals + for CBS will likely be energy depleted, and here
supplementation (in relation to your COMT/VDR status) with Co-Enzyme Q10,
Carnitine, Ribose, and NADH or NAD+ may be helpful.
BHMT (Betaine Homocysteine Methyl Transferase, a zinc-dependent enzyme) directly methylates homocysteine back in to methionine, serving as a “back door” pathway to “pull” homocysteine away from the CBS “sulfate drain”. Thus if you bear CBS or BHMT abnormalities, it makes sense to support BHMT function. TMG (trimethylglycine) stimulate BHMT, and can be utilized if you are not overly sensitive to methyl group supplementation (but you likely are due to your COMT +/+ status). Phosphatidylserine stimulates BHMT (and we also use it to moderate elevated cortisol levels), as does phosphatidylcholine (which we use to treat atherosclerosis). Phosphatidylcholine can be admixed with EDTA (detoxifies metals), creating a quite useful supplement.
Many of you with CBS and BHMT abnormalities will also bear MTHFR (compromising methyl-folate generation) and MTRR (compromising methyl-B12) abnormalities, and thus you will need and benefit from corresponding supplementation (with these molecules that you are having trouble making). However, if we treat you with methyl-folate, methy-B12, or BH4, before we have the CBS problem under control (lower your sulfate status such that glutathione and cysteine assimilation improves) then we will be subjecting you to “incomplete detoxification”. You will feel great for 1-2 days, as beneficial neurotransmitters are generated. Methyl-folate and methyl-B12 detox pathways will then open up, creating toxic intermediates that cannot be metabolized further due to the block in glutathione utilization – and you will feel horrible. Thus we need to resist the temptation to treat your MTHFR/MTRR abnormalities until CBS/BHMT are under control. You’ve lived your entire life with a gene set that is maladaptive to the toxic environment of modern man. It will take us some time to change your internal environment to “bypass” these genomic challenges.
Plan of action for CBS +/- (BHMT discussed further in other
sections)
To address this constellation of alleles I will recommend:
1. Moderate* animal protein intake (anything with eyes) and avoid sulfur rich
vegetables, sulfur containing supplements, and sulfur containing drugs (see
attached sulfur avoidance instruction sheets and read Sulfites and Chronic
Disease by Rick Williams, available at the office or at
www.readingtarget.com/nosulfites/. Basically, from the Methyl Cycle
perspective, returning to a vegetarian diet makes sense for you.
2. Check the sulfate/sulfite content of your supplements and prescription agents
(many listed in the Williams book) and whenever possible switch to agents with
lower sulfate/sulfite content. Some of your current supplements may contain
sulfhydryl groups; all have health benefits but all add to your sulfite/sulfate
burden. We may or may not wish to stop these agents, and results of urine
sulfate testing will help with decision making here.
3. Monitor urine sulfate levels every 3-7 days (or when you feel particularly
good or poorly, or after adding a new treatment or changing your diet). Please
chart the levels – this will be our primary measuring stick – our goal is
a urine sulfate of 400 (one yellow and three pink) to 800 (two yellow and two
pink). Low levels will allow an increase in methyl cycle supplementation and
later the addition of BH4 and/or a liberalization of your diet. Conversely,
persistent high sulfate spills indicates that your diet/treatment program needs
further modification.
3. To neutralize ammonia (generated from animal protein), you can use Ammonia
Support RNA ½ dropper with meals and with methyl cycle supplements (relatively
expensive), along with a charcoal supplement at bedtime every other evening,
away from other supplements (magnesium citrate and Vitamin C may be used as
needed to keep the GI tract moving - optimally twice a day - as charcoal may
lead to constipation). Yucca, beginning at ½ capsule, twice a day, (or
sprinkled on food containing protein), may help with ammonia detoxification.
Ornithine/Aspartate 1000-3000 mg three times a day (taken away from other
sources of protein) will stimulate the urea cycle, promoting ammonia
degradation, and should increase your energy level. While your ammonia level
was not elevated, BH4 is used up in ammonia metabolism, so the less ammonia
formed the better.
4. Sparga Detox, 10 drops in water (wait at least one minute before consuming),
twice a day makes sense (already on board). Sparga was developed by fellow
Cardiologist Dr. Lee Cowden, specifically to address the CBS abnormality (see
www.nutramedix.ec).
5. With respect to overall nutritional support, you and Dr. Smith have the bases
covered based upon your NutrEval study. Could you please send me a treatment
list with mg/mcg doses? Are you taking in riboflavin? If not please add 50-100
mg/day to your program. To stimulate SUOX, please add molybdenum 500 mcg daily
to complement the boron, hydroxy-B12, and boron, which are already present in
your program.
6. Glutathione supplementation runs the risk off adding to your sulfite/sulfate
burden. Right now this “good thing” could actually set you back. However, if
we could convince your biochemistry to up regulate biosynthesis of glutathione,
then your anti-oxidant and detox capacity will increase, with concomitant
utilization of free sulfate/sulfhydryl groups – a double win for you. This can
be achieved with the use of the Life Wave (needleless acupuncture) Glutathione
patch. The Life Wave people have demonstrated an increase in Glutathione levels
in relation to patch use. Please see separate information sheet on Life Wave
patch use; be very conservative early on. This approach may be added in the
future, after your CBS/BHMT situation has been addressed.
7. If you feel anxious or “wired up” (glutamate overload), take GABA 500 mg,
twice a day. If this is helpful you can double the dose. GABA does not work
rapidly, but if you take it twice a day you will build up a GABA reserve to
balance the glutamate overload you are experiencing due to your CBS up
regulation. Magnesium supplementation may help with GABA physiology and often
helps with sleep and is already on board.
8. Regarding energy production, Co-Enzyme Q 50 mg odd days and carnitine 500 mg
even days (we start slow here as these agents are methyl donors). NADH 5 mg/day
(NAD+ might be even more effective) sometimes helps. A trial of ribose 5 gm in
water two to three times a day makes sense; a positive response indicates that
you are having trouble generating ATP energy.
9. After sulfate levels have fallen (to a level that you and I feel is optimal
for you, based upon your clinical and genomic status), then we may increase
methyl-folate and/or add BH4 to your program. While normally I do not start
methyl-folate and methyl-B12 until sulfate levels have fallen. If you are
already on methyl-folate, I do not think they need to be stopped unless urine
sulfate levels remain high and/or you do not improve clinically.
11. I can’t back this up with a clinical study, but the use of Aura Organ Detox
patches for two months make sense. The idea here is not to remove the toxins
(hard to do) but to homeopathically neutralize them). Later, after your sulfate
levels have fallen, we will begin to remove the toxins themselves.
12. With respect to lab testing, we need to check homocysteine now along with a
repeat Vitamin D level. After you have been on your program for 4-6 weeks, we
can measure SAMe and SAH. The Health Diagnostics and Research Institute
(www.hdri-usa.com - $350) can give us levels of SAMe, SAH, and folic acid
derivatives (which will help us understand the affects of your MTHFD, MTHFS, and
DHFR alleles). Alternately, Doctors Data gives us a less extensive but still
useful Methylation Panel for $155.
13. Be self-observant and keep records. Which foods, supplements, or other
maneuvers increase or decrease your sulfate spill? Which make you feel better
or worse? Always keep in mind that detoxification is not a fun experience. You
may need to accept some transient fatigue, malaise, and achiness to allow toxic
molecules to be cleared. Conversely, if detox symptoms are debilitating or
compromise your ability to work or care for your family, then we need to back
off on your treatments. Balance needs to be achieved. Rectifying your genomic
predispositions and detoxifying your system is not a sprint – it is a marathon.
And, as your genes are not going to change, and as the environment is not going
to become less toxic, you will need to be mindful of these principles for the
rest of your (long and healthy) life.
* How tightly should you restrict dietary protein? The
degree of protein restriction best suited for you will be in relation to your
personal health characteristics and your clinical and biochemical (urine sulfate
and ammonia levels) response to treatment. We need to keep in mind that Methyl
Cycle Genomics is not the sole determinant of your health. A low protein diet
can become a high carbohydrate, weight gaining diet in an overweight individual
with type two diabetes. Individuals with chronic, unexplained illness or
significant toxicity would do well to follow the “nothing with eyes” diet until
urine sulfate and ammonia levels have fallen; later on we will liberalize your
diet, while keeping an eye on these biochemical markers. This dietary maneuver
isn’t fun but may also turn one’s your health around. Individuals in whom the
CBS up regulation is less important (A360A as opposed to C677T, lower urine
sulfate and ammonia levels, and better overall health), could simply cut back on
animal protein. In addition, the greater representation of ammonia reducing
(Yucca, Charcoal, Sparga, Ammonia Support RNA) treatments in your program, the
more protein you will be able to take in without compromising your
biochemistry. This is all about balancing diet against treatment response.
** The point of Methyl Cycle analysis/treatment is to help
you become a more efficient detoxifier. Toxicity testing (discussed in more
detail in our Approaches to Detoxification brochure and on heartfixer.com) thus
makes sense. You have already undergone toxicity testing. Additional toxicity
testing could consist of:
A. The US BioTek study gives us information on seven major organic pollutants
($126). The NutrEval tells us that you bear an organic pollutant burden, which
we can address in the future, but I feel that mercury will be out first detox
priority.
B. A formal provocative challenge ($250) gives us our best assessment of tissue
metal burden. Alternatively, an oral DMPS challenge could be carried out, but I
do not feel this is necessary as your red cell mercury level serves as a target
for intervention.
C. The Hunt Digital picture approach ($350) assesses for toxicity (and other
health challenges) by analyzing the frequencies emitted by your body (and tells
us which Digital Homeopathic Patches would be most appropriate). I can’t prove
this approach with an allopathic lab test but it has been quite helpful in
solving complex medical problems in my personal patients. Dr. Hunts CD is
available for your review and you can go to www.auraexplorationpatches.com for
additional information.
D. While on the subject of energy medicine, learn about the
grounding/earthing concept. This approach is low in cost and likely has value
for all of us. My colleague Dr. Sinatra wrote a book on this subject
(heartmdinstitute.com).
OUR MOST IMPORTANT INITIAL GOAL WILL BE TO
REDUCE YOUR SULFATE, AMMONIA, and GLUTAMATE BURDENS
Gene by Gene Approach – COMT +/+ with VDR Taq +/- and MTRR +/-
This constellation of alleles is discussed on pages 193-196
of Dr. Yasko’s book, Genetic Bypass. Being COMT +/+ means that you are
breaking down dopamine, and in the process using up free methyl groups, only
slowly, in your long-term favor with respect to dealing with heavy metals and
microbes. This also means that you will be sensitive to methyl groups, creating
a “treatment conflict”. You may need methyl-B12 due to your MTRR status, but
the extra methyl groups could cause a rise in dopamine, leading to mood swings.
Being +/- for VDR Taq means that Vitamin D will not increase dopamine levels in
the normal fashion, somewhat mitigating this sensitivity to methyl groups, but
we do not need to give you dopamine precursors and we will be on the watch for
mood swings as we give you supplements containing methyl groups. Lithium and
iodine may be lost (swept out) in the process of heavy metal detoxification.
These minerals are felt to help balance or mitigate mood swings that might occur
as a result of fluctuations in dopamine levels, so low dose supplementation
makes sense in COMT +/+ individuals.
COMT (Catechol-O-Methyl Transferase) inactivates catecholamines (dopamine,
norepinephrine, and epinephrine). Caffeine and stress increase catecholamine
production. Individuals with genomic or acquired COMT dysfunction are thus more
sensitive to their effects. Stated otherwise, high coffee intake increases
cardiovascular risk in COMT +/+ individuals but not in those with normal COMT
status, and caffeine induced insomnia will be more of an issue in those with
COMT +/+. COMT is also involved in estrogen metabolism, mediating generation of
the anti-cancer, anti-vascular disease 2-methoxy estrogens and inactivation of
the stronger, potentially genotoxic 4-hydroxy and 16-hydroxy estrogen
molecules.
CYP1A2 +/+ (down regulation) status means that your ability to 2-hydroxylate estrogen molecules will be compromised, while your CYP1B1 +/- (up regulation) status promotes conversion of estrogens down the 4-hydroxylation pathway. Dr. May has you on I3C to stimulate 2-hydroxylation and your 2/16 ratio is thus OK at 2.8.
CYP1A2 +/+ (down regulation) status also compromises your ability to degrade caffeine, which itself stimulates the adrenal gland to release catecholamines, which in turn must be broken down by COMT, the function of which in you (+/+ for the reduced function alleles) is compromised. Thus in your situation caffeine avoidance will be important.
Your COMT +/+ status also explains why your 2-methoxyestradiol levels are relatively low (you are having trouble tacking on the methyl group). This is certainly difficult biochemistry; please see the Estrogen Metabolism section of the website for more information on Estrogen Metabolism and how we can affect it).
Endogenous and caffeine induced catecholamines, estrogen
molecules, and quercetin “compete” for COMT mediated methylation. This is not
an issue in COMT -/- individuals, as there is plenty of COMT function to go
around, but when COMT function is limited (COMT +/+ individuals have only 25%
the O-methylating capacity of COMT -/- individuals), competition becomes more of
an issue. This explains how stress and caffeine increases risk of
cardiovascular disease and reproductive organ malignancy to different degrees in
different people (genomic-environment interaction). COMT +/+ status is also
associated with increased sensitivity to pain.
While estrogens, quercetin, and catecholamines “compete” for the attention of
COMT,
S-Adenosyl Homocysteine (SAH) serves as a “non-competitive” COMT inhibitor.
S-Adenosyl Methionine (SAMe) donates the methyl group that COMT uses to
O-methylate its substrate, producing an O-methylated substrate and SAH. SAMe
and SAH compete for the SAMe binding site on the COMT molecule (think of the
SAMe binding site as the “on-off” switch for COMT). A build up of SAH will thus
turn down COMT activity. When Homocysteine builds up, SAH builds up behind it.
COMT metabolic dysfunction, with secondary inability to metabolize
catecholamines and estrogen molecules, is a key mechanism through which elevated
homocysteine damages our health. Unmetabolized catecholamines and estrogen
molecules generate oxidative stress, leading to vascular and neurological
disease. Unmetabolized estrogen molecules damage DNA, increasing risk of breast
and prostate malignancy. While elevated Homocysteine is always deleterious to
overall health, high Homocysteine in the presence of COMT dysfunction is a
disaster (we will check your homocysteine level and my prediction is that it
will be low).
COMT +/+ individuals cannot utilize methyl groups efficiently, and thus excess methyl group supplementation may lead to irritability in COMT +/+ individuals. Dr, Yasko feels that VDR status effects dopamine generation. Individuals who harbor VDR Taq or VDR Bsm alleles will make less dopamine, and with less dopamine floating around, impaired dopamine inactivation due to one’s COMT +/+ or +/- status becomes less of an issue, and one will be less sensitive to methyl group donors. From the perspective of mood and childhood neurodevelopmental conditions, while COMT +/+ or +/- status renders one sensitive to methyl group supplementation, this is neutralized by VDR +/+ or +/- status.
MTR uses 5-methyl folate and methyl-B12 to convert homocysteine in to methionine. The MTRR abnormality (+/- means that ½ of your MTRR enzymes will work poorly while +/+ would signify that all of your MTRR enzymes would be affected) means that you will have trouble converting B12 in to methyl-B12. Stated otherwise, while your serum B12 level may be “within normal limits”, it will not work normally within your biochemistry. As you are COMT +/+ and VDR +/- you will be sensitive to methyl groups. Thus we will start not with methyl-B12, but with high doses of hydroxy-B12, aiming for the hydroxy-B12 to bind with the methyl groups available to form methyl-B12. If we do not feel that this approach is getting the job done, we could add in methyl-B12 cautiously, watching for mood swings. B12 methylation does not appear to be a problem for you, as your methionine and methylmalonic acid levels are OK.
By stimulating BHMT, we can bypass any block that MTRR places on homocysteine detoxification, and this maneuver will also draw methyl cycle intermediates away from sulfate/sulfite production. Phosphatidylserine and phosphatidylcholine stimulate BHMT and makes sense. Lipophos EDTA provides phosphatidyl choline to stimulate BHMT and EDTA to remove lead (which compromises function of multiple enzymes, whether they are genetically normal or abnormal, including GAD, which converts glutamate in to GABA). TMG (trimethylglycine) will stimulate BHMT but will also provide methyl groups, to which you are likely sensitive, and is thus best avoided.
If agitation or anxiety is an issue (perhaps on the basis of excessive glutamate production due to a CBS up regulation), we can address this with GABA 500 mg, 1-2 twice a day. We need glutamate for learning and alertness, but excessive glutamate leads to “excitotoxicity”, manifested clinically as agitation and anxiety and pathologically as neural damage. Conversely, GABA counterbalances glutamate, providing a calming effect (all drugs of the valium class stimulate the GABA receptor). We should be able to interconvert glutamate, alpha-ketoglutarate, and GABA, but the enzymes systems involved in this process are sensitive to heavy metals, likely a problem in you. GABA does not work quickly, or “as needed”, but if taken twice a day your GABA pool will increase such that stress tolerance and your overall sense of well being should improve. GABA should not produce excessive drowsiness, lethargy, or dependency (as valium class drugs may). Zen contains GABA and theanine, another GABA agonist, but theanine provides methyl groups, to which you are sensitive, so for you GABA alone is a better choice. Other approaches to dealing with an imbalance between glutamate and GABA include avoiding glutamate rich food products (see list) and supplementation with grape seed extract 100 mg/day (taurine helps here but might aggravate your CBS/sulfite overload situation). Lipophos EDTA provides phosphatidyl choline to stimulate BHMT and EDTA to remove lead (which compromises function of multiple enzymes, whether they are genetically normal or abnormal, including GAD, which converts glutamate in to GABA). EDTA efficiently removes lead and cadmium, and has activity against aluminum, nickel, and arsenic. EDTA is not an efficient mercury chelator. EDTA is typically well tolerated in individuals with a CBS up regulation.
Lithium and iodine may be lost (swept out) in the process of heavy metal detoxification. These minerals are felt to help balance or mitigate mood swings that might occur as a result of fluctuations in dopamine levels, so low dose supplementation makes sense in COMT +/+ individuals, with dosing guided by blood levels. Unless we are taking in iodized table salt, most of us in non-coastal regions will be iodine deficient, compromising or metabolism and possibly thyroid function. Iodine supplementation may improve thyroid function, while paradoxically, in some individuals, excessive iodine may compromise thyroid function or induce thyroiditis (I’ve seen this). Thus it makes sense to check thyroid chemistries several months after beginning iodine supplementation, particularly if you are receiving thyroid hormone supplementation.
Dr. Yasko’s RNA products, to my knowledge, are “silencing” or “interference” RNAs, which affect the reading of your DNA in a fashion beneficial for specific genomic challenges. They are expensive, and proof of efficacy has not been provided (and we do not hold this against Dr. Yasko as proving anything in biological medicine costs millions of dollars). Their inclusion in your program is ideal but adds significantly to your costs, so from my perspective their use can be deferred (or added later if our initial approaches are not getting the job done).
Plan of action for COMT +/+ with VDR Taq +/- , and MTRR +/-
1. Sublingual
Hydroxy-B12 is already on board to stimulate SUOX and seems to be covering your
MTRR +/- status. Before switching to methyl-B12 (which you probably do not need)
I would like to measure your SAMe level with the Doctor’s Date methylation panel
(in 8 weeks).
2. Lithium Orotate 5 mg alternating with Iodoral three days a week (Sundays off)
makes sense, with plans to obtain a 24 hour urine mineral assessment and serum
iodine level in 8 weeks..
3. To stimulate BHMT and spare BH4, phosphatidyl choline (PhosChol) 900 mg/day
makes sense. If PhosChol agrees with you (most patients feel better on
PhosChol) the dose could be advanced to 900 mg twice a day (more on this in the
Methyl Thieves section). Soy bean lecithin 1-2 tablespoons/day would serve as a
lower cost alternative to PhosChol.
4. When you and Dr. Smith feel you are physiologically strong enough for metal
detoxification, we could utilize a program of Lipophos EDTA (stimulates BHMT and
pulls out metals) ¼ bottle twice a week in juice (we may later increase to ½
bottle twice a week), with Phosphatidylcholine 900-1800 mg the remaining five
days of the week.
5. Limit supplements that provide methyl groups, such as melatonin, turmeric,
theanine, and MSM, as we need to “make room” for methyl-B12.
6. We need to check you vitamin D level.
7. Methylation support RNA ¼ dropper per day would be ideal here (and expensive
and thus not critical).
If you feel poorly, this could represent allergy/intolerance to one of your therapies, the effects of excessive methyl groups (despite our biochemical precautions), but more likely this will represent a detox reaction, as dammed up toxins start leaving your body. This is not a negative – we want you to detoxify. However, if a detox reaction is compromising your functional status, we can back off on your program, and then resume at a lower dose when you are feeling better. You are entering this process because your health has been compromised and allopathic (drugs and surgery) medicine has not helped you, and thus you may need to endure some short-term discomfort to achieve your long-term goal (a return of good health).
MTR (Methionine Synthase) transfers a methyl group from Methyl-folate to
Homocysteine to form Methionine.
MTRR (Methionine Synthase Reductase) adds the Methyl group to otherwise inactive
B-12.
BHMT (Betaine-Homocysteine Methyltransferase) mediates the “backdoor” pathway of
homocysteine metabolism, directly methylating homocysteine back to SAMe.
COMT (Catechol-O-Methyl Transferase) breaks down dopamine and norepinephrine and
to a somewhat lesser extent other neurotransmitter substances, by tacking on to
them a free methyl group that COMT obtains from
SAMe.
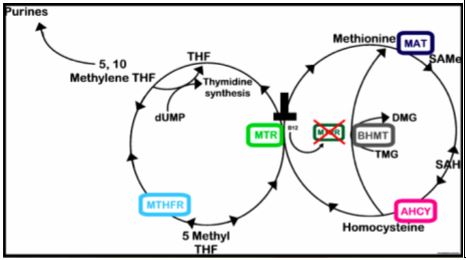
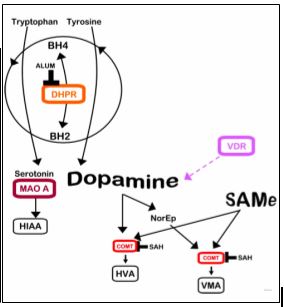
|
COMT V158M (+/+) |
Highest dopamine levels |
|
COMT V158M (-/-) |
Lowest dopamine levels |
Gene by Gene Approach and Plan of Action – MTHFR A1298C +/+
Dr. Yasko describes MTHFR A1298C as an abnormality in the SAMe binding site of MTHFR that compromises the “backward reaction” that generates BH4, a problem in that BH4 is being used up detoxifying ammonia (which you are making in excess due to your CBS up regulations). This “backward reaction” is not supported by other authors, but a pathway does exist (mediated by DHFR) such that poor methyl-folate status will compromise BH4 recycling. Methyl folate supplementation may stimulate the backward reaction and will help regenerate BH4, and methyl-folate can “stand in” for BH4 when the latter is depleted. After your urine sulfate levels have fallen we may advance methyl-folate or add in BH4 supplementation. If we supplement aggressively in the presence of high urine sulfate, patients may feel great for one day and then experience an incomplete detox reaction. As you are already on methyl-folate I do not think you need to stop it but we will not increase the dose until sulfate levels are under control (< 800). Sauna increases BH4 production and promotes detoxification and could be utilized.
Gene by Gene Approach – SHMT +/-
SHMT combines the amino acid serine with folic acid to form 5,10-methylene THF, which is used to generate the building blocks for DNA and RNA generation. We can bypass this block with 5-formyl THF, also known as Folinic acid.
Plan of Action – SHMT +/-
As you are +/- and not +/+ for SHMT please add 5-formyl THF, also known as folinic acid, 400 mcg daily (or 800 mcg every other day) to your program.
Gene by Gene Approach and Plan of Action – DHFR +/-
Here you are having some trouble reducing oxidized dietary folates into useful Tetrahydrofolate, and in recycling “spent” BH2 back in to useful BH4. Our approach here involves methyl-folate and folinic acid supplementation, as discussed above.
Gene by Gene Approach and Plan of Action – FOLR2 +/+
To some degree, your cellular folate receptors are having trouble incorporating folic acid. This is probably less of an issue with methyl-folate. You may need more methyl-folate than others. Our approach here is general support of the Methyl Cycle and the inclusion of methyl folate in your program.
Gene by Gene Approach and Plan of Action – MTHFD1 G1958A +/+
The trifuncitonal enzyme, 5,10-methylenetetrahydrofolate dehydrogenase/ 5,10-methylenyltetrahydrofolate cyclohydrolase/ 10-formyltetrahydrofolate synthetase (MTHFD1) is responsible for the conversion of 5,10-methylene THF (generated from THF by SHMT) to the corresponding 10-formyl, 5,10-methenyl and 5,10-methylene derivatives. A common mutation at position 1958 within the MTHFD1 gene results in a transition of guanine to adenine (G>A) that may result in a reduction in folate metabolism. Our approach here involves general support of the Methyl Cycle and the inclusion of methyl-folate and folinic acid in to your program. The Health Diagnostics and Research Institute (www.hdri-usa.com - $350) can give us levels of SAMe, SAH, and folic acid derivatives (which will help us understand the affects of your SHMT, MTHFD, MTHFR, and DHFR alleles).
Gene by Gene Approach – MAO A +/+
MAO breaks down serotonin and
to a lesser extent dopamine and norepinephrine. This disorder is associated
with an increased tendency to mood swings and panic disorders, related to
fluctuations in serotonin levels. Serotonin formation may pick up as BH4 levels
are restored with other maneuvers to address methyl cycle abnormalities.
Tryptophan in food is converted into serotonin and tyrosine in food in to
dopamine. As you are +/+ for COMT and have a high urine dopamine, you do not
need to emphasize with tyrosine or tryptophan rich foods in your diet (and our
initial goal is to lower sulfate, so our key dietary recommendation is to avoid
animal protein). Progesterone may stimulate MAO A activity.
Gene by Gene Approach – Methyl Thieves and SAMe Stealers
A key goal of Methyl Cycle physiology (and a focus in our work with you) is to
ensure sufficient, replenishable, and physiologic (not excessive) supplies of:
A. SAMe, along with and an appropriate SAMe to SAH ratio (it is the ratio, not
just the SAMe level, that drives forward useful methylation reactions).
B. BH4 (needed to generate neurotransmitters and nitric oxide), and
C. Key antioxidant and detoxification molecules (glutathione, taurine, sulfate,
and cysteine).
You are generating (or taking) methyl folate and methyl B12, not for the sake of
generating high levels of these Methyl Cycle intermediates (yes, intermediates,
not finished products), but rather to help ensure that the Methyl Cycle work
products (SAMe, BH4, glutathione, cysteine, and taurine) are in adequate supply.
While our focus has been on improving SAMe supply, we should also consider means
to reduce SAMe expenditure (Mother Nature balances supply and demand – the
government should pay heed)! Stated otherwise, if nutritional supplementation
decreases demand for SAMe, more will be available to meet critical demands (e.g.
DNA methylation to silence inflammatory and proto-oncogenes).
So how are we “spending” SAMe? What phenomena lead to SAMe wasting or
diversion? How do we ameliorate these pathophysiologies to restore SAMe and
appropriate SAMe:SAH balance?
In considering SAMe expenditure, remember that each time we
“spend” a SAMe (S-Adenosylmethionine) to carry out a specific methylation
reaction, we create a SAH
(S-Adenosylhomocysteine), which in turn inhibits methylation. A declining
SAMe:SAH inhibits methylation reactions; it does us no good to increase SAMe if
at the same time we buildup SAH.
Fortunately, SAH is rapidly converted to Homocysteine and Adenosine. Adenosine is efficiently removed, but if the Methyl Cycle is sluggish, due either to SNIPS, toxins, or nutritional deficiency, Homocysteine will build up. Homocysteine will then be back converted to SAH, the SAMe:SAH ratio falls, and useful methylation grinds to a halt. Homocysteine itself is not the problem; it is the buildup of SAH, compromising methylation potential, which leads to disease states such as atherosclerosis, cancer, and mood disorders.
So what processes “steal” SAMe? In considering this issue, we need to be aware
that CBS (which irreversible drains Homocysteine down the trans-sulfuration
pathway and away from SAMe reformation) is up regulated (enzymatic activity
increases) by oxidative stress and inflammation.
A. Oxidative stress:
When the generation of free radicals (superoxide, hydroxyl, and hydrogen
peroxide) outpaces our ability to neutralize them with endogenous (e.g.
superoxide dismutase) or exogenous (supplemental antioxidants), we suffers from
a buildup of free radicals. To address this immediate threat to health,
Homocysteine metabolism down the CBS pathway (irrespective of SNIP status) will
increase. Homocysteine (and with it the potential to create new SAMe) will be
irreversibly diverted away from remethylation (via MTR and BHMT back into
methionine for conversion to SAMe) and towards the production of glutathione,
taurine, and cysteine.
This all makes sense. Oxidative stress damages our physiology and kills cells. When faced with oxidative death, it makes sense to divert Methyl Cycle resources towards antioxidant generation. After oxidative stress has been neutralized, CBS flow will decrease, Homocysteine will start flowing back towards SAMe, and useful methylation reactions will resume. Our problem is that most ill Americans suffer from unremitting oxidative stress (we can measure your individual level of oxidative stress with the NutrEval study). Homocysteine will thus be shunted down the CBS pathway, such that useful methylation of DNA, estrogen molecules, and catecholamines will be compromised. If you cannot methylate catecholamines, then oxidative stress will develop within your blood vessels. If you cannot methylate your DNA, than you cannot silence inflammatory genes. You thus make more inflammatory molecules, more free radicals build up, more Homocysteine is diverted away from SAMe regeneration, and you are now chronically ill.
The solution is to undergo an assessment of oxidative stress, and then takes steps to resolve any challenges present. This will involve removing from your body phenomena that generate free radicals (e.g. smoking, toxic metals, organic pollutants) while concomitantly shoring up your antioxidant defenses with nutrients that we find to be in short supply (selenium, Vitamin E, Vitamin C, etc.). We can thus use nutritional medicine to help you generate SAME and to prevent oxidative stress from “stealing” Homocysteine away from SAMe regeneration. As a side note, toxic metals not only “steal” SAMe, they also compromise its formation (e.g. Mercury compromises MTR, in this fashion blocking useful remethylation of Homocysteine back into methionine for conversion into SAMe). Other than a mild depression in glutathione your oxidative stress/inflammatory markers were within the reference range. Your SOD2 +/+ status compromises superoxide dismutase and thus your ability to degrade the free radical superoxide, which we can address with GliSODin supplementation. Being +/- for GSTP1 and GPX1 you are having some trouble utilizing glutathione. As residual heavy metals are removed, there will be less strain on your glutathione stores. Paraoxonase is involved in organic pollutant metabolism; it also provides the antioxidant activity of HDL and is involved in the metabolism of homocysteine thiolactone. Pomegranate juice intake makes sense to stimulate paraoxonase (you are +/- for a loss of function PON allele).
B. Inflammation: Inflammatory TH1/TH17 cytokines, such as TNF-alpha, Il-6,
and Il-1b also increase flow down the
CBS pathway, draining Homocysteine away from useful remethylation back in to
SAMe. Inflammation leads to oxidative stress and oxidative stress leads to
inflammation. Both are useful in fighting infection, but both processes are
persistently elevated as our immune system misinterprets as infection the
chronic “pseudoinfections” of visceral obesity, leaky gut, and environmental
toxicity. Thus by resolving inflammation (either with anti-inflammatory
nutrition interventions such as turmeric or berberine) or by removing the cause
of chronic inflammation (weight loss or resolving leaky gut) we can resolve the
“inflammatory drain” on SAMe supply and demand.
What processes deplete our SAMe stores? Are some less critical than others? Can we decrease SAMe demand with nutritional supplementation?
A. DNA methylation: This is sacrosanct. Only SAMe can methylate DNA. Only SAMe can shut down the transcription (reading into protein formation) of viral, inflammatory, and proto-oncogenes (promote cancerous transformation) while maintaining the transcription of tumor suppressing and anti-inflammatory genes. We can’t scrimp on DNA methylation, but by resolving oxidative/inflammatory stress, and supplementing with SAMe “sparers” as described below, we can maintain adequate SAMe (with a high SAMe:SAH ratio) to ensure optimal DNA methylation.
B. Creatine formation: Around 50% of our SAMe is “spent” in the generation of creatine, a molecule critical to energy maintenance. We do work by splitting a high energy bond within ATP (Adenosine Triphosphate) to produce ADP and phosphate. We burn carbon and use this energy to rephosphorylate ATP. When energy is plentiful, ATP will transfer a phosphorus group to creatine, forming Phosphocreatine. Should we suddenly run out of ATP energy (sprinting, weight lifting, or if oxygen supply:demand is compromised by a blocked artery or failing heart), Phosphocreatine can download a high energy phosphate bond back to ADP, regenerating ATP such that cellular work can continue. We actually store 10 heart beats of energy as Phosphocreatine. As you would expect, creatine supplementation has been shown to be helpful in anaerobic athletic performance as well as in heart failure. Of interest, creatine has been shown to lower cholesterol, and while the literature is not 100% consistent, creatine supplementation will decrease expenditure of SAMe and increase the SAMe:SAH ratio. Creatine lowers homocysteine in individuals with MTHFR abnormalities. Athletes take 5 grams of creatine, four times a day (saturation dose) for one week, followed by 5 grams/day (maintenance dose). However, unless you have an athletic competition coming up, you can simply add 5 grams of creatine/day to your program. Creatine is not unsafe, but there have been instances where competitive body builders dosed up on creatine while decreasing fluid intake (so their muscles will bulge out more) leading to dehydration and kidney compromise. Creatine is converted in to Creatinine, which is filtered out by the kidneys. We use serum creatinine to gauge kidney function. A trivial rise in serum creatine may occur when you supplement with creatine. This does not mean that kidney function is decreasing; rather this is an artifact due to creatine supplementation. Creatine supplementation at 5 grams/day makes sense for individuals with Methyl Cycle SNIPS that might compromise SAMe generation or maintenance (MTHFR, MTR, CBS, and BHMT), or when we feel that chronic oxidative/inflammatory stress is depleting SAMe regeneration.
C. Phosphatidylcholine: Three SAMe molecules, around 30% of our total supply, are used to methylate phosphoethanolamine into phosphatidylcholine. Phosphatidylcholine (PC) is involved in lipoprotein formation and reverse cholesterol transport; PC is also a critical component of the cell membrane. The common name for PC is lecithin. PC/lecithin is essentially a triglyceride like molecule with two fatty acids and one phosphocholine group attached to a three carbon glycerol backbone. The biochemical utility of PC relates to the composition of its two fatty acids. PC containing two unsaturated linoleic acid molecules (polyenylphosphatidylcholine) is used IV and orally to treat cardiovascular, liver, and neurological disease (see our DVD presentation). If we supplement you with PC, less SAMe will be spent generating PC, and more will be available for useful methylation reactions. In addition, the less SAMe spent, the less SAH and Homocysteine will be formed. Furthermore, PC can be converted into choline, which can be converted into Betaine (TMG or trimethylglycine) which is used by BHMT to directly remethylated homocysteine back in to methionine (which is then converted in to SAMe). Thus PC supplementation will lower an elevated Homocysteine and increase SAMe supply along with the SAMe:SAH ratio. We use PhosChol (unsaturated phosphatidylcholine rich in linoleic acid) 900 to 2700 mg/day in the treatment of cardiovascular and liver disease. Our dose in Methyl Cycle patients will relate to your SNIP status and baseline Homocysteine level.
Being +/+ for PEMT, you are having trouble generating phosphatidylcholine.
PEMT is stimulated by estradiol and this may explain why homocysteine levels
rise when ovarian hormone levels decline. Phosphatidylcholine supplementation
will bypass your PEMT status and spare SAMe, a double win for you.
D. COMT utilization. COMT (Catechol-O-Methyl transferase) metabolizes estrogen molecules, catecholamines (dopamine and norepinephrine), drugs (e.g. L-Dopa used in the treatment of Parkinson’s disease) and bioflavonoids (particularly Quercetin) by transferring a methyl group from SAMe to an oxygen molecule on the compound being methylated. Each time this occurs, SAH is generated, the SAMe:SAH ratio falls, and COMT and all other methyl-transferase enzymes are inhibited. If we are interested in sparing SAMe and maintaining a high SAMe;SAH ratio, it would be prudent to reduce the need for COMT-driven methylation. Lowering stress will lower norepinephrine, and thus decrease SAMe utilization by COMT. While bioflavonoids such as Quercetin have many beneficial properties, if SAMe preservation is critical (high Homocysteine in the presence of MTHFR, MTR, MTRR, and BHMT SNIPs or if our ability to methylate estrogen molecules is impaired) then decreasing intake of Quercetin and related bioflavonoids would be prudent. Conversely, when insufficient dopamine is the problem, we might use Quercetin to blunt dopamine degradation by “clogging up” COMT. Caffeine increases catecholamine production. Caffeine intolerant individuals are typically COMT +. When caffeine intolerance develops anew, we look for new problems that might be compromising SAMe supply or COMT functionality.
Plan of action
for Methyl Thieves and SAMe Stealers )
1. Creatine 5 gm/day makes sense.
2. PhosChol at 900 mg/day, advancing to 900 mg twice a day if the initial dose
of 900 mg daily agrees with you.
3. Pomegranate juice 1 oz/day (Pom Wonderful was used in the cardiovascular
research, with positive effects).
4. GliSODin 250 mg/day would be ideal.
Gene by Gene Approach and Plan of Action – AHCY +/-
SAMe is converted in to S-adenosylhomocysteine, which is converted in to homocysteine by AHCY. Being +/- for AHCY, you may be having trouble with SAH degradation. We address this alleles with general support of the Methyl Cycle and measures to ensure that Homocysteine levels are not elevated
Additional Thoughts
1. My
hypothesis is that your Methyl Cycle abnormalities have rendered you more
susceptible to metal toxicity, while at the same time sensitive to side-effects
with the use of our –SH based mercury detox agents (why you felt poorly with IV
DMPS). When you and Dr. Smith feel you are ready, then further metal
detoxification makes sense. Matching detox therapies to the individual patient
is sort of an art of medicine concept. The Hunt aura patch approach is
typically well tolerated and a good place to start. A negative field only sleep
pad is of value to all but quite expensive. Grounding is inexpensive and
reasonable. Foot bath/sauna therapy is also typically well tolerated. Our
standard mercury chelators (DMSA and DMPS) are sulfite-rich and would likely not
be tolerated, while EDTA based preparations (good for lead, cadmium, and
aluminum) would likely be reasonably well tolerated (and later we could return
for mercury using a non-sulfhydryl based therapy). Please look through our
Detoxification Options brochure. I just came across Dr. Chi’s approach to metal
overload and his brochure is enclosed
2. Regarding the recurrent viral outbreaks the Aura OLE patch might work. The
digital picture analysis will tell us if the corresponding frequency is present.
3. Please forward to me a current treatment list, with doses in mg or mcg units.
4. Please run all of this by Dr. Smith (who will receive a copy of this report,
and you have given me permission to consult with her regarding your care), and
we can certainly discuss all of the above during a phone conference.).
James C. Roberts MD FACC FAARFM 1/18/15
Sample Report - Adult with Atherosclerosis
|
Methyl Cycle Nutrigenomic Report |
||
|
Methylation Panel Abnormalities for Genes with Characterized SNPs |
||
|
Gene Name |
Variation |
Finding |
|
COMT |
V158M |
OK |
|
COMT |
H62H |
OK |
|
COMT |
61 |
OK |
|
VDR |
Bsm |
OK |
|
VDR |
Taq |
Homozygous (+/+) |
|
MAO A |
R297R |
Homozygous (+/+) |
|
ACAT |
102 |
OK |
|
MTHFR |
C677T |
Heterozygous (+/-) |
|
MTHFR |
3 |
OK |
|
MTHFR |
A1298C |
OK |
|
MTR |
A2756G |
OK |
|
MTRR |
A66G |
Heterozygous (+/-) |
|
MTRR |
H595Y |
OK |
|
MTRR |
K350A |
OK |
|
MTRR |
R415T |
OK |
|
MTRR |
A664A |
OK |
|
BHMT |
2 |
OK |
|
BHMT |
4 |
OK |
|
BHMT |
8 |
OK |
|
AHCY |
1 |
OK |
|
AHCY |
2 |
OK |
|
AHCY |
19 |
OK |
|
CBS |
C699T |
Heterozygous (+/-) |
|
CBS |
A360A |
Heterozygous (+/-) |
|
CBS |
N212N |
OK |
|
SHMT |
C1420T |
Heterozygous (+/-) |
Overview
You are +/- for both of the CBS up regulations. Homocysteine (and its Methyl Cycle precursors) is thus being drawn down the trans-sulfuration pathway, in this process generating excessive sulfur breakdown products (sulfite and sulfate – and your urine sulfate is 1600 - which stimulate the stress/cortisol “fight or flight” response), too much alpha-ketoglutarate (which may lead to glutaminergic excitotoxin activation), and too much ammonia, which depletes BH4, leading to insufficient dopamine and serotonin production. This deficiency in BH4 predisposes NOS (nitric oxide synthase) to convert Arginine in to free radicals as opposed to nitric oxide, predisposing you to hypertension and cardiovascular disease. You are already on BH4 and methyl-folate, and after the up regulated trans-sulfuration pathway (CBS) has come under control, the BH4 and methyl-folate doses could be increased.
CBS actually
generates sulfite, which must be processed to sulfate, by SUOX (sulfite
oxidase). Even thought your urine sulfite level is normal, support for this
enzyme with hydroxy-B12, molybdenum, boron, and Vitamin E succinate can be
considered.
MTR uses 5-methyl folate and methyl-B12 to convert homocysteine in to
methionine, which is then converted in to SAMe, the universal methyl donor. You
are +/- for MTHFR C677T, meaning that you have some difficulty converting folic
acid in to 5-methyl folate, a block that is (biochemically) easy to overcome
with 5-methyl folate supplementation (already in place).
You are also +/- for one of the MTRR alleles, meaning that you are having some trouble converting B12 in to methyl-B12, a problem that you have already addressed with methyl-B12 supplementation. You are +/+ for VDR Taq, such that Vitamin D will be less efficient in generating dopamine, and -/- for COMT, meaning that you can breakdown dopamine rapidly, using up methyl groups in doing so, and thus you will have an increased susceptibility to toxic metals and viral infection. Conversely, your need and tolerance for methyl groups and methyl donors will be relatively increased (your problem is not sensitivity to methyl donors but rather sensitivity to sulfites/ammonia/glutamate that are generated when these agents spin forward the Methyl Cycle and homocysteine is drawn down the up regulated CBS “drain”).
SHMT combines the amino acid
serine with folic acid to form 5,10-methylene THF, which is used to generate the
building blocks for DNA and RNA generation. We can bypass this block with
5,10-methylene THF, also known as Folinic acid.
Being +/+ for MAO A, you are having trouble breaking down serotonin, an issue
that we can address by favoring foods rich in tyrosine, the precursor to
dopamine, which you need, over foods rich in tryptophan, the precursor for
serotonin. Early on, however, an overall restriction of dietary animal protein
will be suggested, to decrease the ammonia burden imposed on you by your CBS up
regulation status.
My knowledge
of Detoxification Genomics is far less extensive than that of the Methyl Cycle,
but my understanding is that the CYP1B1 alleles present are an up regulation,
favoring 4-hydroxyglation of estradiol/estrone, thus increasing one’s risk of
breast/prostate malignancy. Hydrocarbon pollutants are activated by 1B1, and if
they cannot be neutralized by phase II enzyme systems, oxidative tissue damage
may follow. CYP2C19 metabolizes a number of commonly utilized pharmaceuticals,
and is also responsible for activating Plavix. Thus you may not be experiencing
the same anti-platelet effect vs. an individual with intact 2C19 status (likely
not an issue now, one year out from stent placement, but if another stent is
required one of the newer agents that does not require 2C19 activation would be
preferred). Methylation based (COMT) phase II detoxification is intact, but you
harbor alleles compromising acetylation and SOD (superoxide dismutase)
generation (thus neutralization of superoxide will be compromised, but on board
you have SOD up regulators in the form of Losartan, Crestor, and Berberine).
The Gene by Gene Approach sections provide general information about the alleles
you possess, while the Plan of Action sections contain specific
recommendations. Approaches that make the most sense to me receive a (Ö).
Those that are less critical (or more costly) are designated (+/-). Based upon
review of your medical history, I have a number of additional diagnostic and
therapeutic ideas (please see below).
Gene by Gene Approach – CBS +/-
CBS (Cystathionine Beta-Synthase) is discussed on pages 48-53 of Dr. Yasko’s
book, Genetic Bypass. Additional information is available on our heartfixer.com
website. You are +/- (half of your CBS enzymes abnormal) for both of the two
CBS up regulations. Fortunately you are -/- (normal function or “wild type”)
for the BHMT down regulations (which act like CBS up regulations). Given your
CBS up regulations, Homocysteine (and its Methyl Cycle precursors) is being
drawn down the trans-sulfuration pathway, in this process generating excessive
sulfur break down products (sulfite and sulfate, which stimulate the stress/cortisol
“fight or flight” response), too much alpha-ketoglutarate (which leads to
glutaminergic excitotoxicity), hydrogen sulfide (to produce brain fog), and too
much ammonia (which depletes BH4, leading to insufficient dopamine and serotonin
production). This deficiency in BH4 allows NOS (nitric oxide synthase) to
convert arginine in to free radicals (superoxide and peroxynitrite) as opposed
to nitric oxide, predisposing you to hypertension, cardiovascular and
inflammatory disease states.
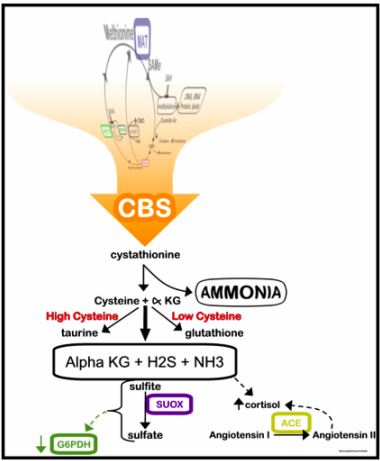
During normal physiology, metabolic flow down the CBS pathway is designed to generate the important anti-oxidant and detoxifying molecules glutathione, taurine and cysteine (all involved in detoxification and endothelial health), and alpha-ketoglutarate (which can be converted into GABA, a calming neurotransmitter). The CBS C677T and A360A genes code for enzyme function that is pathologically up regulated. Of the two, the C677T allele is the most important, producing enzyme activity that is 10 fold greater than normal. You thus suffer from “too much of a good thing and way too much of several bad things”.
While sulfate and sulfhydryl (-SH) bearing molecules are important in detoxification, sulfate/sulfite/-SH excess blocks cellular up take of the key detoxifiers glutathione and cysteine. Endogenous detoxification is thus blunted (nearly all kids with Autism Spectrum Disorders bear CBS up regulations – why they are compromised by environmental toxins and the kid next door is just fine). Conversely, after we decrease your sulfate/sulfite pool, your detox pathways open up (and why, if we move too fast, you will experience detox phenomena).
The excess ammonia generated must be detoxified, and to do so BH4 (tetrahydrobiopterin) must be “spent”. This is a problem in that we need BH4 to generate neurotransmitters (serotonin to maintain calm/prevent depression and dopamine to maintain motivation and drive). Without BH4, we cannot convert arginine in to nitric oxide; instead vascular wall toxic free radicals such as superoxide and peroxynitrite are created, leading to hypertension and cardiovascular disease.
Alpha-ketoglutarate, in
moderation, is not a problem. We should be able to interconvert
alpha-ketoglutarate into glutamate, glutamine, and GABA. However, when
alpha-ketoglutarate is in excess, or if toxic metals compromise the
interconversion enzymes, then we suffer a buildup of the excitatory
neurotransmitter glutamate. Glutamate is involved in alertness and learning,
but excess glutamate leads to irritability and over-excitement; toxic levels may
play a role in seizure activity and cardiac arrhythmia (could this be why we are
seeing so much atrial fibrillation)?
CBS up regulations lead to an initial buildup of potentially neurotoxic sulfite,
which is then metabolized by SUOX (Sulfite Oxidase) to the less neurotoxic (but
still problematic at high levels) sulfate. SUOX activity requires molybdenum,
which is thus depleted in CBS + individuals. Homogenized dairy products contain
xanthine oxidase, which uses up molybdenum, and are best avoided or minimized.
Vitamin E succinate, boron, and B12 are felt to stimulate SUOX activity.
As methyl cycle function is needed in the biosynthesis of Co-Enzyme Q10 and Carnitine, individuals + for CBS will likely be energy depleted, and here supplementation (in relation to your COMT/VDR status) with Co-Enzyme Q10, Carnitine, and NADH may be helpful.
Statin therapy predictably depletes Co-Enzyme Q; adding 100-200 mg/day of Co-Enzyme Q makes sense or we could measure your Co-Q level with a Genova Labs NutrEval study.
BHMT (Betaine Homocysteine Methyl Transferase) directly methylates homocysteine back in to methionine, serving as a “back door” pathway to “pull” homocysteine away from the CBS “sulfate drain”. Thus if you bear CBS or BHMT abnormalities, it makes sense to support BHMT function. DMG (dimethylglycine) and TMG (trimethylglycine) stimulate BHMT, and can be utilized if you are not overly sensitive to methyl group supplementation (based upon you COMT/VDR status). Phosphatidylserine stimulates BHMT (and we also use it to moderate elevated cortisol levels), as does phosphatidylcholine (which we use to treat atherosclerosis). Phosphatidylcholine can be admixed with EDTA (detoxifies metals), creating a quite useful supplement.
Many of you with CBS and BHMT
abnormalities will also bear MTHFR (compromising methyl-folate generation) and
MTRR (compromising methyl-B12) abnormalities, and thus you will need and benefit
from corresponding supplementation (with these molecules that they are having
trouble making). However, if we treat you with methyl-folate, methy-B12, or
BH4, before we have the CBS problem under control (sulfite/sulfate levels
decreased enough to allow for appropriate glutathione and cysteine assimilation)
then we will be subjecting you to “incomplete detoxification”. You will feel
great for 1-2 days, as beneficial neurotransmitters are generated.
Methyl-folate and methyl-B12 detox pathways will then open up, creating toxic
intermediates that cannot be metabolized further due to the block in glutathione
utilization – and you will feel horrible. Thus we need to resist the temptation
to treat your MTHFR/MTRR abnormalities until CBS/BHMT are under control.
However, you are already on methyl-folate, methyl-B12, and BH4 and I do not
think that you need to stop them simply on the basis of this “new Methyl Cycle
patient” principle.
Plan of action for CBS +/-
To address this constellation of alleles I will recommend:
1. Moderate* animal protein intake (anything with eyes) and avoid sulfur rich
vegetables, sulfur containing supplements, and sulfur containing drugs (see
attached sulfur avoidance instruction sheets and read Sulfites and Chronic
Disease by Rick Williams, available at the office or at
www.readingtarget.com/nosulfites/.
2. Check the sulfate/sulfite content of your supplements and prescription agents
(many listed in the Williams book) and whenever possible switch to agents with
lower sulfate/sulfite content.
3. Monitor urine sulfate levels every 3-7 days (or when you feel particularly
good or poorly, or after adding a new treatment or changing your diet). Please
chart the levels – this will be our primary measuring stick – our goal is
a urine sulfate of 400 (one yellow and three pink) to 800 (two yellow and two
pink). Low levels will allow an increase in methyl cycle supplementation and
later the addition of BH4 and/or a liberalization of your diet. Conversely,
persistent high sulfate spills indicates that your diet/treatment program needs
further modification.
3. To neutralize ammonia (generated from animal protein), you can use Ammonia
Support RNA ½ dropper with meals and with methyl cycle supplements (relatively
expensive), along with a charcoal supplement at bedtime every other evening,
away from other supplements (magnesium citrate may be used as needed to keep the
GI tract moving as charcoal may lead to constipation). Yucca, beginning at ½
capsule, twice a day, (or sprinkled on food containing protein), may help with
ammonia detoxification. These supplements can be tapered down as ammonia levels
fall.
4. Sparga Detox, 10 drops in water (wait at least one minute before consuming),
twice a day makes sense. Sparga was developed by fellow Cardiologist Dr. Lee
Cowden, specifically to address the CBS abnormality (see www.nutramedix.ec).
5. For nutritional support, a low-sulfate multi such as Dr. Yasko’s Neurological
Health Formula, 3-6/day, makes sense (or we may have you on another preparation
in relation to your other health concerns). To stimulate SUOX activity, please
use sublingual hydroxy-B12 2000 mcg/day, along with Molybdenum and Boron. They
may be taken individually as Molybdenum 3 drops in water twice a day and Boron 3
mg once a day, while our Complete Mineral Complex, 3 daily will cover the
mineral base. Avoid B6 (unless you need it for other functions), which
stimulates CBS. The active form of B6, P-5-P, is less of a problem here and
serves as a B6 substitute.
6. Glutathione supplementation runs the risk off adding to your sulfite/sulfate burden. Right now this “good thing” could actually set you back. However, if we could convince your biochemistry to up regulate biosynthesis of glutathione, then your anti-oxidant and detox capacity will increase, with concomitant utilization of free sulfate/sulfhydryl groups – a double win for you. This can be achieved with the use of the Life Wave (needleless acupuncture) Glutathione patch. The Life Wave people have demonstrated an increase in Glutathione levels in relation to patch use (please see separate information sheet on Life Wave patch use).
7. If you feel anxious or “wired up” (glutamate overload),
take GABA 500 mg or Zen (GABA 550 mg with Theanine 200 mg, a methyl donor) twice
a day. Individuals who need methyl groups (normal COMT and/or abnormal VDR Taq
alleles – your situation) will do better with Zen, while individuals who are
methyl group sensitive (COMT+) will likely do better with GABA. If they are
helpful you can double the dose. GABA/Zen do not work rapidly, but if you take
these supplements twice a day you will build up a GABA reserve to balance the
glutamate overload you may be experiencing due to your CBS up regulation.
Magnesium supplementation may help with GABA physiology and often helps with
sleep.
8. If energy is low, or if deficiencies are identified on your NutrEval study,
we can supplement you with Co-Enzyme Q and Carnitine. NADH does not provide
methyl groups and should be well tolerate by all.
9. What is your homocysteine level? A low level suggests that your CBS up
regulation is of great functional significance, with a homocysteine “drain”
overcoming the MTHFR and MTRR abnormalities (which otherwise would be associated
with an elevated homocysteine level). If not previously measured we should
check it now. Further nutritional testing can be carried out in 8-12 weeks.
This could involve separate 24 hour urine studies for nutritional minerals and
for ammonia/amino acids, or we could use the Genova Labs NutrEval. We need to
make sure your mineral/nutritional stores are replete, and we are looking for
low levels of ammonia, taurine, glutamate, and cysteine, to demonstrate that
flow down the CBS pathway has been decreased to a physiologic level.
10. After sulfate levels have fallen (to a level that you and I feel is optimal
for you, based upon your clinical and genomic status), we could advance
supplementation with methyl-folate, methyl-B12, and BH4 (nutritional testing
will help with decision making here).
11. A key goal of Methyl Cycle analysis is to improve your
ability to detoxify, and thus toxicity testing** (which you have already
undergone) and treatment make sense. I can’t back this up with a clinical
study, but the use of Aura Organ Detox patches for two months may help you.
This approach does not remove toxins but is felt to homeopathically neutralize
them). Later, after your sulfate levels have fallen, we can take further aim at
the toxins themselves. Dr. Hunt’s CD is available for your review and you can
go to www.auraexplorationpatches.com for additional information. This approach
has been helpful when I have been stumped despite a full allopathic laboratory
work up, and I am now liberal with its use.
12. Sauna therapy increases BH4 production and promotes detoxification, and
could be utilized (low exposure at first, watching for detox reactions).
Footbath therapy is another means of removing toxins without adding foreign
molecules to your body.
11. Be self-observant and keep records. Which foods, supplements, or other
maneuvers increase or decrease your sulfate spill? Which make you feel better
or worse? Always keep in mind that detoxification is not a fun experience. You
may need to accept some transient fatigue, malaise, and achiness to allow toxic
molecules to be cleared. Conversely, if detox symptoms are debilitating or
compromise your ability to work or care for your family, then we need to back
off on your treatments. Balance needs to be achieved. Rectifying your genomic
predispositions and detoxifying your system is not a sprint – it is a marathon.
And, as your genes are not going to change, and as the environment is not going
to become less toxic, you will need to be mindful of these principles for the
rest of your (long and healthy) life.
* How tightly should you restrict dietary protein? The
degree of protein restriction best suited for you will be in relation to your
personal health characteristics and your clinical and biochemical (urine sulfate
and ammonia levels) response to treatment. We need to keep in mind that Methyl
Cycle Genomics is not the sole determinant of your health. A low protein diet
can become a high carbohydrate, weight gaining diet in an overweight individual
with type two diabetes. Individuals with chronic, unexplained illness or
significant toxicity would do well to follow the “nothing with eyes” diet until
urine sulfate and ammonia levels have fallen; later on we will liberalize your
diet, while keeping an eye on these biochemical markers. This dietary maneuver
isn’t fun but may also turn one’s your health around. Individuals in whom the
CBS up regulation is less important (A360A as opposed to C677T, lower urine
sulfate and ammonia levels, and better overall health), could simply cut back on
animal protein. In addition, the greater representation of ammonia reducing
(Yucca, Charcoal, Sparga, Ammonia Support RNA) treatments in your program, the
more protein you will be able to take in without compromising your
biochemistry. This is all about balancing diet against treatment response.
** The point of Methyl Cycle analysis/treatment is to help you become
a more efficient detoxifier. Toxicity testing (discussed in more detail in
other presentations and on heartfixer.com) thus makes sense. You have already
undergone toxicity testing (and I would like to review with you the results).
Testing options for new patients include:
A. The NutrEval provides us some information regarding organic pollutants and
gives us red cell (reflecting what your physiology has been exposed to over the
preceding three months) toxic metals ($170 with commercial insurance; fully
covered under non-HMO Medicare).
B. The US BioTek study gives us information on seven major organic pollutants
($126); this is less extensive than the Metametrix study that you have already
carried out and will not add any new information.
C. A formal provocative challenge ($250) gives us our best assessment of tissue
metal burden.
D. The Hunt Digital picture approach ($350) assesses for toxicity (and other
health challenges) by analyzing the frequencies emitted by your body (and tells
us which Digital Homeopathic Patches would be most appropriate). I can’t prove
this approach with an allopathic lab test but it has been quite helpful in
solving complex medical problems in my personal patients. Dr. Hunts CD is
available for your review and you can go to www.auraexplorationpatches.com for
additional information.
OUR MOST IMPORTANT INITIAL GOAL WILL BE TO
REDUCE YOUR SULFATE STORES
Gene by Gene Approach – COMT -/- with VDR Taq +/+ and MTRR +/- or +/+
This constellation of alleles is discussed on pages 112-115
of Dr. Yasko’s book, Genetic Bypass. Additional information is available on our
heartfixer.com website. VDR Taq influences dopamine production. Being +/+ for
VDR Taq means that dopamine production is compromised. Being COMT -/- means
that you are breaking down dopamine rapidly and in doing so using up available
methyl groups, compromising your ability to deal with toxins and microbes (thus
you are more likely than COMT +/- or COMT +/+ individuals to bear a metal
burden). You need and should tolerate dopamine precursors and methyl donors.
MTR uses 5-methyl folate and methyl-B12 to convert homocysteine in to
methionine. Being MTRR +/- or +/+, you are having trouble converting B12 into
methyl-B12, a problem that is biochemically easy to overcome with methyl-B12
supplementation.
As you are COMT -/- and VDR +/+ you should tolerate methyl group
supplementation reasonable well, so begin supplementation with methyl-B12
(already on board) with a plan to increase the dose to 5 mg per day after urine
sulfate levels have fallen. Why wait for sulfate to fall? Methyl-B12
supplementation, by moving the cycle of homocysteine metabolism forward, could
lead to increased ammonia and sulfite/sulfate generation, so normally we do not
push with methyl-B12 until urine sulfate levels have decreased. If you
possessed normal CBS alleles, then sulfate generation is not an issue, but you
harbor a genomic challenged in this pathway and thus we need to move slowly with
respect to methyl-B12 (and methyl-folate) supplementation.
As you are COMT -/- and VDR +/+, you are making less
dopamine in response to
Vitamin D and you are breaking dopamine down rapidly. Thus you need and should
tolerate methyl donors such as Methyl-B12, TMG, melatonin, curcumin, SAMe, or
MSM (hold off on MSM if urine sulfate levels are high). You might benefit from
quercetin and macuna puriens, both of which support dopamine production, or
Procite-D, which does the same
By stimulating BHMT, we can bypass any block that MTRR places on homocysteine detoxification, and this maneuver will also draw methyl cycle intermediates away from sulfate/sulfite production. Pedi-Activ contains phosphatidyl serine, which stimulates BHMT, and DMAE, a methyl donor, and its use makes sense. Lipophos Forte provides phosphatidyl choline which stimulates BHMT. Lipophos EDTA provides phosphatidyl choline to stimulate BHMT and EDTA to remove lead (which compromises function of multiple enzymes, whether they are genetically normal or abnormal, including GAD, which converts glutamate in to GABA) and cadmium (which contributes to hypertension and cancer risk).
If you are troubled by agitation or anxiety (perhaps on the basis of excessive glutamate production due to a CBS up regulation), we can address this with GABA or Zen (GABA + Theanine). As you are COMT -/- and VDR Taq +/+, you should tolerate and benefit from the methyl groups provided by theanine. However, if agitation occurs, suggesting methyl group excess, we can utilize GABA, which does not contain methyl groups (both GABA and theanine stimulate the GABA receptor, and thus provide a “Valium” like effect without concern for drowsiness or dependency). Neither GABA or Zen work quickly (we have other supplements for “as needed” use) and are best taken twice a day as a nutritional approach to combat the biochemical consequences of stress (emotional or glutamate-induced stress). Other approaches to dealing with an imbalance between glutamate and GABA include avoiding glutamate rich food products (see website) and supplementation with grape seed extract 100 mg/day and/or (if a CBS up regulation is not present) taurine 500 -1000 mg/day. Lipophos EDTA provides phosphatidyl choline to stimulate BHMT and EDTA to remove lead (which compromises function of multiple enzymes, whether they are genetically normal or abnormal, including GAD, which converts glutamate in to GABA). EDTA efficiently removes lead and cadmium, and has activity against aluminum, nickel, and arsenic. EDTA is not an efficient mercury chelator. EDTA is typically well tolerated in individuals with a CBS up regulation.
Plan of action for COMT -/- with VDR Taq +/+, and MTRR +/-
1. Methyl-B12
is already present at 1,000 mcg daily; please advance to 5,000 mcg daily after
urine sulfate levels have fallen to 800 (or if subsequent testing indicates an
increased need for B12 nutriture).
2. Quercetin + daily to provide methyl group, antioxidant, and dopamine support
makes sense; ginkgo biloba, macuna puriens, and Procite-D serve as alternative
approaches to augment dopamine status.
3. Unless agitation (suggesting too many free methyl groups) occurs, you may
supplement freely with methyl donors such as melatonin, curcumin, TMG, or SAMe).
3. Lipophos Forte 900 mg (one teaspoon) daily mixed in juice or Phosphatidyl
serine can be utilized to stimulate the BHMT pathway (unsaturated
phosphatidylcholine has anti-atherosclerotic activity and of the two is thus
preferred). Alternatively, if metal detoxification is appropriate, Lipophos
EDTA ½ - ½ bottles twice a week can be matched with Lipophos Forte five days a
week.
4. Zen (GABA and the methyl donor theanine) twice a day if anxiety or agitation
is an issue for you.
5. Supplement to keep Vitamin D » 50.
6. At some point in the future, after urine sulfate levels have declined, try
adding SAMe 200 mg/day to your program. While we would prefer that you generate
SAMe endogenously, exogenous SAMe will provide methylation support and with your
COMT -/- and VDT+R Taq +/+ status you should tolerate it
well.
MTR (Methionine Synthase) transfers a methyl group from Methyl-folate to Homocysteine to form Methionine. MTRR (Methionine Synthase Reductase) adds the Methyl group to otherwise inactive B-12. MTRR abnormalities compromise the generation of methyl-12. Without methyl-B12, MTR cannot use methyl-folate to recycle homocysteine into methionine.
VDR Taq +/+ or +/- (impaired) status compromises the production of dopamine. COMT -/- (normal function) allows rapid breakdown of the dopamine you can generate. VDR Taq+/+ with COMT -/- individuals will experience low dopamine levels (with consequent increased sensitivity to metal overload) and will benefit from dopamine precursor therapy and from methyl group donors.
|
COMT V158M (+/+) |
Highest dopamine levels |
|
COMT V158M (-/-) |
Lowest dopamine levels |
Gene by Gene Approach – MTHFR C677T +/-
Here the MTHFR enzyme present is having trouble converting folic acid into 5-methyl folate. Without 5-mehtyl folate MTR cannot detoxify homocysteine in to methionine. 5-methyl folate has another role here - it can neutralize peroxynitrite. When NOS (nitric oxide synthase) is not functioning normally (i.e. when BH4 is deficient), arginine is converted not into the vasoprotective molecule nitric oxide, but rather into the damaging free radicals superoxide and peroxynitrite. Superoxide (neutralized by Vitamin C) can further degrade nitric oxide, while peroxynitrite degrades BH4 (stimulating a vicious cycle). 5-methyl folate can neutralize peroxynitrite, thus sparing BH4, keeping it available such that NOS can generate nitric oxide, the vasoprotective molecule that we need - thus the need to maintain healthy production/levels of 5-methyl folate. We can easily bypass the MTHFR C677T block with 5-methyl folate supplementation. Sources of 5-methyl folate include Folapro (800 mcg 5-methyl folate), Metanx (5-methyl folate 2.8 mg, P5P 25 mg, and methyl-B12 2 mg), and Cerafolin NAC (5-methyl folate 5.6 mg, NAC 500 mg, and methyl-B12 2 mg).
Plan of Action – MTHFR C677T +/-
Please continue with methyl-folate at 1,000 mcg per day; after urine sulfate levels fall we will advance the dose (and possibly advance BH4).
Gene by Gene Approach – SHMT +/-
SHMT combines the amino acid serine with folic acid to form 5,10-methylene THF, which is used to generate the building blocks for DNA and RNA generation. We can bypass this block with 5,10-methylene THF, also known as Folinic acid.
Plan of Action – SHMT +/-
Begin Folinic Acid 800 mcg/day; this should not produce any tolerance issues.
Gene by Gene Approach – MAO A +/+
MAO breaks down serotonin and to a lesser extent dopamine and norepinephrine.
This disorder is associated with an increased tendency to mood swings and panic
disorders, related to fluctuations in serotonin levels. Serotonin formation may
pick up as BH4 levels are restored with other maneuvers to address methyl cycle
abnormalities. Tryptophan in food is converted into serotonin and tyrosine in
food in to dopamine. If one is abnormal for MAO and normal for COMT, then
emphasizing foods higher in tyrosine (see Appendix I) than in tryptophan makes
sense (however, our initial goal is to lower sulfate, so the recommendation to
avoid animal protein overrides the recommendation to take in foods high in
tyrosine).
Additional Thoughts
1. You have
likely undergone an extensive nutritional/risk factor/toxicity work up, but if
you have not I have the following thoughts -
A. With respect to atherosclerosis, please check:
a. Lp(a), and if at all elevated begin Lp(a) neutralizing therapy with lysine,
proline, and additional Vitamin C.
b. Free testosterone and estradiol, and if no prostate contraindications
supplement to obtain high normal free testosterone and low normal estradiol
levels.
c. Fibrinogen – if high you can use turmeric or nattokinase to lower the level
and thus blood viscosity.
d. Ferritin (predominately under genomic control), and if elevated undergo
periodic phlebotomy/give blood to the Red Cross, aiming for a ferritin
» 100.
e. EndoPAT endothelial function testing, and if subpar you could advance
Arginine further (most clinical trials used 2-,4000 mg two to three times a day)
or add in Citrulline (likely boosts intracellular arginine).
B. With respect to atherosclerosis management, immune modulation could be added
to your program (particular is CRP or other inflammatory markers are elevated).
Proven approaches include Pentoxifylline (please see DVD) and Colchicine (best
article attached). Testosterone works within this framework as well.
C. With
respect to organic pollutant detoxification, the following detox modalities are
available:
a. Far Infrared Sauna – detox at home while watching the playoffs.
b. Footbath therapy – the Ion Cleanse people demonstrated that organic materials
are removed with their device. As the principle involved is common to all of
the devices available, most likely they all are effective. We have switched to
the Platinum Footbath device which seems to be more effective and user
friendly. This approach can be used at home as well.
C. The best approach is supplementation with agents that up regulate phase I and
to a greater extent phase II. All contain sulfhydryl donors (sometimes a
problem is CBS + individuals), but if tolerance is not an issue, an effective
approach would be to carry out a 10 day organic pollutant detox, three times a
year, utilizing the Metagenics Clear Change program (other nutraceutical
companies have similar programs), with an agent such as Metagenics Metalloclear
or Glutaclear (up regulate detox/antioxidant pathways – incidentally Berberine
also does this) when not on the Clear Change program. You could repeat the
Metametrix pollutant panel in the future; the Genova NutrEval gives similar but
less extensive information regarding organic pollutant burden (and if covered
under Medicare).
D. Regarding metals, in TACT we demonstrated that old-fashioned, one size fits all EDTA chelation therapy improves outcome when added to standard post-infarction management. Stated otherwise, metals seem to be playing an important role in the oxidative stress and immune dysregulation that characterize atherosclerosis. In your case, IV EDTA is the most powerful approach to lead and cadmium removal, while Lipophos EDTA will up regulate your BHMT pathway and unsaturated phosphatidylcholine (please see DVD) has an anti-atherosclerotic effect. However, EDTA is a poor mercury chelator. Here we typically use oral DMSA or IV or topical DMPS, but both are sulfhydryl group rich, and might not be well tolerated, given your CBS + status. This creates a treatment dilemma – these agents you need are the ones you tolerate the least. Here you could try DMSA, three times a day, three days in a row, once a month, beginning at 100 mg and working up to 500 mg, and you might tolerate it well. Static magnetic field therapy seems to synergize with biochemical chelation and is a thought (I have been sleeping on a negative filed sleep pad over the past 10 years). In DMSA/DMPS intolerant individuals, another approach involves the use of QuickSilver resin or Pectasol (modified citrus pectin – please see econeugenics.com).
E. Regarding CYP1B1 and the risk of malignancy, Genova has a urine estrone/estradiol hydroxylation/methylation study. If 1B1 is functionally significant, your ration of 4-OH to 2-OH will be high. This can be rectified with 1B1 down regulators and 1A1 (promotes 2-hydroxylation) up regulators such as DIM or I3C (please see Estrogen Metabolism section on the website).
2. Attached are DVDs, information sheets, and papers pertaining to the topics discussed above.
3. We could
carry out a phone consultation regarding the above if you wish, and/or carry out
the diagnostic studies listed above. I am happy to help in any
capacity.
James C. Roberts MD FACC FAARFM 1/4/14
The Life Wave patches utilize a needless acupuncture concept to favorably influence physiology. The science and clinical studies underlying this concept can be reviewed at lifewave.com/chc, which we encourage you to study. No physical molecules leave the patch (in contrast to a Nitropatch or an Estrogen patch); they are technically described as “non-transdermal”. The Life Wave patches are not homeopathic (as are the Aura patches that we also use). The Life Wave patches do not spontaneously emit energies; rather they absorb frequencies emanating from your body and then selectively return some of them. When you place a patch on or near your body, frequencies leaving your body cause the molecules within the patch to self-assemble in to a crystal structure. The crystal structure serves as an antenna, capturing frequencies leaving your body (kind of like a FM receiver), and then, depending on the function of the patch, it selectively emanates frequencies into the Meridian communication system, as a function of where on the system the patch is placed. Energy flow within the Meridian system is increased, directing your body to carry out actions that it currently is not carrying out, or not carrying out efficiently. The Life Wave patch is like a program that we insert into your computer to make certain programs run more efficiently.
Each type of patch comes with step by step instructions. We can increase the cost-effectiveness of this system. The instructions tell you to discard a patch after it has been removed; however, each patch appears to be able to work for 48 hours of contact time. The patch is activated when it is placed on or near your body (so do not carry them around in your pocket). It inactivates when it is removed. So if a patch works over 48 hours, you could wear it 48 hours straight, or you could wear it for 6 hours/day over 8 days (adhesive tape may be needed).
The most important patch is the Y-Age Glutathione patch. This patch directs your body to manufacture more glutathione, using raw materials already present and your body’s own enzyme systems. Glutathione is the key antioxidant/detoxification molecule in your body. Conversely, glutathione depletion occurs in response to chronic oxidative stress and toxicity (as in the average American). IV administration of glutathione increases excretion of toxic substances. Oral glutathione is not absorbed; instead we give your its precursor substance N-Acetyl Cysteine (used in Medicine to prevent kidney failure during angiographic procedures, tolerance to long-acting nitrates, or liver failure in Tylenol overdose situations). Those of you with the Methyl Cycle Cystathionine Beta Synthase (CBS) up regulation will not tolerate N-Acetyl Cysteine (due to its Sulfur content), but you should have no trouble with the patch. The patch does not provide you with Sulfur-containing molecules; rather it directs you to assemble these molecules into glutathione, a molecule that you can put to good use and a molecule that you likely need.
A note of caution - If you wear the patch glutathione production will increase, and if you are loaded with toxins – then you will begin to detoxify. Drink plenty of water to facilitate this process, and if you feel poorly simply remove the patch – then put it back on the next day (it should give your 48 hours of service). If you are vigorous and healthy, you will likely be able to wear the patch for 6-8 hours on your first day, but if you are ill, you might want to try only 2-4 hours on your first day, and then gradually increase your “patch on” time on a day-by-day basis. Another issue, Vitamin C and N-Acetyl Cysteine both resolve Nitrate tolerance (loss of clinical effect due to Nitrate-induced glutathione depletion), and when we use these agents we sometimes have to back off on your Nitrate dose. The same may occur with the patch - a “good problem”.
The pain patch system is a little different. Place the tan patch over the point of greatest pain, and then the white patch 4-6 inches away. A reduction of pain is typically noted within 10 seconds. Positioning of the white patch can be altered to obtain the best result. In my mind I think of the white patch as “draining pain away” from the tan patch (this isn’t actually what is happening, but the concept helps when considering patch placement). There are also patch placement positions to deal with total body pain. You can wear two sets, one for total body pain and another to address a focal source of pain. You can then place a glutathione patch in the palm of your right hand. If this maneuver lowers pain even more, than it makes sense to wear the glutathione patch, over one of the specific glutathione control points, to augment pain relief. Feel free to experiment with patch positioning. Remember, you do not have to remove the backing of a patch to activate it. It is energy (frequencies) emanating from your body that activate the patch. Wear the pain patches for 48 hours or as you see fit (if the effect attenuates at 24-36 hours, then replace the patches on this schedule). If they fall off, then tape them back on. If an injury is minor, then the patches might actually speed up healing (by drawing energy into the region of pain, just as standard needle Acupuncture does). A deep injury is obviously not going to heal with energy flow alone, but if the patch system allows you to use less pain medication, and/or less anti-inflammatory drug therapy, then a goal has been achieved.
The Carnosine patch directs your body to produce carnosine, a powerful
antioxidant. I alternate between the two, glutathione one day and carnosine the
next. We do not yet have any experience with the weight loss or sleep patches.
Regarding the weight patch, Life Wave recommends that you wear the glutathione
patch for 2 months before beginning the weight loss program, the idea being that
your body (in its wisdom) packs fat-soluble toxins like pesticides and
herbicides in to body fat, to protect more important regions (like your nervous
system). When you attempt to lose weight, you may feel poorly, as these toxins
are released. It also may be that your body actively blocks your attempts at
weight loss (by down regulating metabolism) because it wants to protect you from
the release of toxicity (this theory may or may not be true but it makes sense
biologically). In any event, more glutathione cannot be anything but good you.
James C. Roberts MD FACC 5/27/08